
Pitted keratolysis — the foot condition that almost never gets diagnosed correctly on the first visit: Patients describe the smell as unbearable. They’ve tried medicated foot powder, antifungal spray, and multiple pairs of shoes. Nothing works because it isn’t fungus — it’s a bacterial infection that p

- SUPPORTS HEALTHY HAIR (1): Biotin helps maintain healthy hair; providing essential nutrients crucial for beautiful hair (1)
- SKIN AND NAIL HEALTH SUPPORT (1): These Biotin softgels are designed to support hair, skin and nail health (1)
- NERVOUS SYSTEM SUPPORT (1): Biotin supplement; a member of the B Vitamins family; supports a healthy nervous system (1)
- ENERGY METABOLISM BENEFIT (1): Biotin 10000mcg aids in converting nutrients into cellular energy; supporting the body's energy metabolism (1)
- QUALITY YOU CAN TRUST (1): Backed by 50 years of scientific research; these Nature's Bounty biotin vitamins offer a reliable choice for your health and beauty (1)

- REINFORCES THIN NAILS - Sally Hansen's nail strengthener and nail care has all you need for healthy nails
- ONE COAT - Strengthen thin, weak nails with just one coat of our quick-drying nail strengthening polish
- POTECTS FROM BREAKING - With Sally Hansen's Maximum Growth Nail Polish, you'll have stronger nails that are less likely to break or split.
- KEEPING NAILS GROWING - Fortifies and defends nails so they continue to grow
- SILK FORMULA - Triple-protection and silk formula

- Alleviate Discomfort – These flexible corn cushions help reduce rubbing and chafing. Each corn cushion measures approximately 1″ x 3/4′. The hole is approximately 1/4″ in diameter.
- Thick, Supportive Fabric – Toe cushions for corns or calluses are made with a thick, flexible layer that properly covers the affected area for all-day relief.
- Water Resistant Adhesive – The back of each foot corn cushion features a self-sticking callus cover that stays on even if your foot or toes get wet.
- High Quality Materials – Designed with a skin safe latex base, small corn cushions are gentle on sensitive skin and fit men and women equally.
- Improved Foot Comfort – Soft corn cushions fit comfortably inside socks or shoes without bunching, sliding or falling off; even while running or working out.
Few foot conditions cause as much embarrassment — and confusion — as pitted keratolysis. Patients come into our Howell and Bloomfield Hills offices having tried every antifungal cream on the pharmacy shelf with no improvement, convinced they have a fungal infection, when in reality they have a bacterial one. The treatment is completely different, and once the correct diagnosis is made, the response is typically swift and dramatic.
What Is Pitted Keratolysis?
Medically reviewed by Dr. Tom Biernacki, DPM
Board-certified podiatric surgeon | Balance Foot & Ankle
Last reviewed: May 2026
Pitted keratolysis is a superficial bacterial infection of the stratum corneum — the dead outer layer of skin — on the soles and heels of the feet. The bacteria that cause it produce enzymes called proteases that literally digest and crater the keratin (protein) in this thick skin layer, creating the characteristic pits. The bacteria responsible are gram-positive organisms, primarily:
- Corynebacterium species — the most common culprit
- Kytococcus sedentarius (formerly Micrococcus sedentarius)
- Dermatophilus congolensis
- Actinomyces species — less common
These organisms are part of the normal bacterial flora of the skin but proliferate excessively when the environment becomes chronically warm and moist — exactly the conditions inside occlusive footwear worn for hours at a time. The infection is not contagious in the traditional sense; it’s an overgrowth of bacteria that are already present, not a pathogen transmitted from another person (though shared footwear can introduce organisms).
What Does Pitted Keratolysis Look Like?
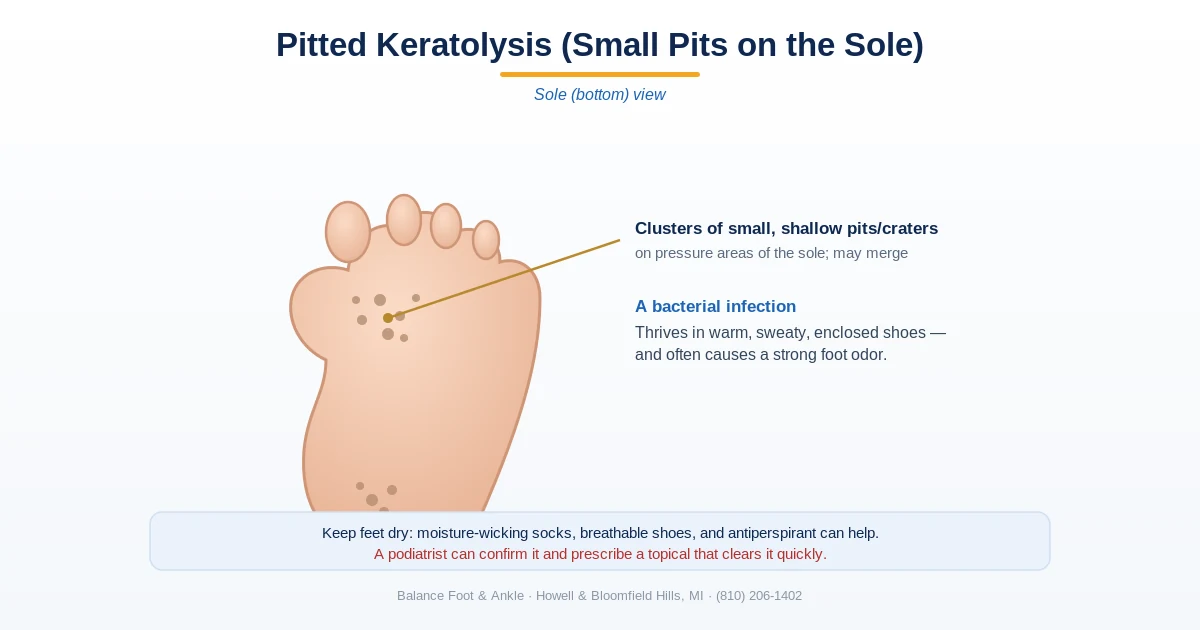
The visual findings are highly distinctive once you know what to look for. The hallmark is small, discrete, crater-like pits (0.5–7 mm in diameter) punched into the thick skin of the weight-bearing areas of the sole — primarily the pressure points: the balls of the feet under the metatarsal heads, the heels, and the toe pads. The pits may be solitary, clustered in groups, or in severe cases so numerous they coalesce into large eroded plaques.
The appearance changes with moisture exposure. When the feet are dry, the pits may appear subtle — small brownish or grayish craters. When wet (after showering, sweating, or swimming), the affected skin turns distinctly white and macerated, and the pits become far more visible. This wet-white appearance is one of the most diagnostically useful features.
In some cases, the skin takes on a slimy or “cheese-like” texture when wet. The surrounding skin may be mildly inflamed, and in longstanding cases the pits can merge into large superficial erosions that make the entire heel or ball of foot look eroded.
Key takeaway: The characteristic odor of pitted keratolysis is produced by sulfur compounds — thiols and sulfides — that the bacteria release as metabolic byproducts when they digest keratin. It is one of the most distinctive and unpleasant odors in dermatology and is diagnostic on its own when combined with the visual pitting.
Who Gets Pitted Keratolysis?
Pitted keratolysis is strikingly common in specific occupational and athletic groups — populations whose feet are consistently enclosed in occlusive footwear for prolonged periods:
- Athletes — runners, soccer and football players, and anyone wearing athletic shoes for hours of daily training
- Military personnel — boots worn for prolonged field operations create ideal bacterial conditions; pitted keratolysis has been reported in 30–40% of some military cohorts
- Manual laborers — construction workers, factory workers, and others in safety boots or rubber-soled work shoes
- Healthcare workers — prolonged shifts in closed-toe nonbreathable footwear
- People with primary hyperhidrosis (excessive sweating) — the elevated baseline moisture dramatically accelerates bacterial proliferation
It is more common in warm, humid climates and in summer months in temperate climates. In our Michigan clinics, we see a spike in presentations from June through September, corresponding to increased sweating in the summer heat.
Key takeaway: Pitted keratolysis is not a fungal infection — it is bacterial. This distinction matters enormously for treatment: antifungal creams like clotrimazole (athlete’s foot treatment) have no effect on pitted keratolysis. Topical antibiotics, specifically clindamycin or erythromycin solution, are the correct treatment and produce rapid clearance.
Diagnosis: How We Confirm It
In most cases, pitted keratolysis is a clinical diagnosis — the characteristic pitting pattern on the pressure-bearing sole, the accompanying malodor, the patient’s history of occlusive footwear and sweating, and the absence of the scaling/blistering pattern typical of tinea pedis are sufficient to make the diagnosis with high confidence.
We do not routinely culture pitted keratolysis — the offending bacteria are difficult to culture and the diagnosis is usually clear without it. However, we will culture if:
- The presentation is atypical (unusual location, severe erosion, systemic symptoms)
- The patient fails standard topical antibiotic therapy after 3–4 weeks
- There is concern for a mixed bacterial infection or secondary cellulitis
A Wood’s lamp examination (ultraviolet light) may show coral-red fluorescence from bacterial porphyrins, though this finding is inconsistent across the causative bacteria. A KOH preparation (potassium hydroxide scraping) is used to rule out tinea pedis — a negative KOH in a patient with pitting strongly supports the bacterial diagnosis over fungal.
The key conditions we differentiate pitted keratolysis from in our workup: tinea pedis (athlete’s foot — scaling and blistering predominate, not pitting; KOH positive), palmoplantar keratoderma (diffuse thickening without discrete pits), dyshidrotic eczema (blistering, intensely itchy, palms often involved), and viral warts (verruca plantaris) (harder central core, disrupts skin lines, no odor).
Treatment: What Actually Works
Treatment targets both the active infection and the moisture environment that sustains it. Both components are required — treating the infection without fixing the moisture problem leads to rapid recurrence.
First-line treatment: Topical antibiotics. The most effective and well-studied treatments are:
- Clindamycin 1% solution or gel — applied twice daily to the affected areas. Highly effective, clears most cases within 2–4 weeks. Available by prescription.
- Erythromycin 2% solution — equivalent efficacy to clindamycin; some patients prefer the formulation. Available by prescription.
- Mupirocin (Bactroban) ointment — effective but less commonly used as first-line; excellent for localized or severe areas.
- Fusidic acid — widely used internationally with good evidence; less available in the US.
Over-the-counter benzoyl peroxide wash (5–10%) has some supporting evidence as adjunctive therapy — it reduces the bacterial load and the odor-producing sulfur compounds directly. Some patients use it as a foot wash while awaiting or during antibiotic therapy.
Antiperspirant for moisture control: This step is as important as the antibiotic. We recommend applying a 20% aluminum chloride solution (prescription Drysol or OTC Certain Dri) to the soles nightly for the first 1–2 weeks, then 2–3 times weekly for maintenance. Aluminum chloride shrinks the sweat gland pores and dramatically reduces the moisture environment that feeds the bacteria.
Oral antibiotics (erythromycin or clindamycin) are reserved for widespread severe cases or patients who cannot reliably apply topical therapy — they are generally not needed for straightforward pitted keratolysis.
Key takeaway: The most important prevention strategy: moisture control. Bacteria that cause pitted keratolysis thrive only in chronically moist environments. Moisture-wicking socks, rotating shoes to allow drying, foot powder (especially aluminum chloride-based antiperspirant), and airing feet after activity interrupt the moisture cycle that feeds the infection.
Prevention: Stopping the Recurrence Cycle
Pitted keratolysis recurs readily when conditions that produced it are not changed. A complete prevention protocol:
- Moisture-wicking socks (merino wool or synthetic moisture-wicking blends) rather than cotton — cotton holds moisture against skin
- Rotate footwear — never wear the same shoes two days in a row; allow 24–48 hours for moisture to evaporate and bacteria to die
- Air feet for 15–30 minutes after removing shoes; sandals when indoors
- Foot powder (talcum or cornstarch-based) applied to the soles and inside shoes each morning
- Breathable footwear — mesh uppers and natural materials when activity permits; avoid rubber or PVC-lined shoes for daily wear
- Continue maintenance antiperspirant 2–3x weekly on the soles even after clinical clearance
For patients with primary hyperhidrosis — excessive sweating that occurs regardless of temperature or activity level — the standard prevention measures may be insufficient. We offer iontophoresis (electrical current passed through water to reduce sweating) and botulinum toxin injections to the plantar surface as more definitive options for this subset of patients.
⚠️ When pitted keratolysis needs professional evaluation
- Pitting that extends beyond the soles to the palms or other body areas — atypical presentation requiring workup
- Failure to improve after 2–3 weeks of topical antibiotic therapy — may need oral antibiotics or culture to identify resistant organism
- Significant pain with weight-bearing — pitted keratolysis is typically painless; pain suggests secondary cellulitis or a different diagnosis
- Systemic symptoms (fever, swollen lymph nodes) alongside the foot findings — bacterial spread beyond skin
- Recurrent pitted keratolysis despite following all prevention measures — consider underlying hyperhidrosis requiring procedural treatment
The Bottom Line
Pitted keratolysis is a common, easily treatable bacterial skin infection of the sole that is frequently misdiagnosed as athlete’s foot and treated with useless antifungal medication. The moment a patient gets a correct diagnosis and starts topical clindamycin plus aluminum chloride antiperspirant, they typically see improvement within days and complete clearance within 3–4 weeks.
If you’ve been treating a persistent foot odor problem or pitting on your soles without success, the most likely reason is that you’re treating the wrong organism. A single podiatric visit in our Howell or Bloomfield Hills office to confirm the diagnosis and prescribe the correct topical antibiotic is usually all it takes.
Get Rid of the Odor and Pitting for Good
Same-day appointments available in Howell & Bloomfield Hills, MI
4.9★ | 1,123 Reviews | 3,000+ Surgeries Performed
Or call: (810) 206-1402
Sources
- Blaise G, Nikkels AF, Hermanns-Le T, et al. Corynebacterium-associated skin infections. Int J Dermatol. 2008;47(9):884-890.
- Longshaw CM, Wright JD, Farrell AM, et al. Kytococcus sedentarius, the organism associated with pitted keratolysis, produces two keratin-degrading enzymes. J Appl Microbiol. 2002;93(5):810-816.
- Makhija M, Bhattacharya SN. Pitted keratolysis revisited. Indian J Dermatol. 2011;56(4):442-443.
- Singh G, Naik CL. Pitted keratolysis. Indian J Dermatol Venereol Leprol. 2005;71(3):213-215.
- Takama H, Tamada Y, Yano K, et al. Pitted keratolysis: clinical manifestations in 53 cases. Br J Dermatol. 1997;137(2):282-285.
Frequently Asked Questions: Pitted Keratolysis
For a complete clinical overview: Our Complete Nail & Skin Conditions Guide — covers toenail and skin infections of the foot with diagnosis and treatment from a Michigan DPM.
According to the National Library of Medicine, pitted keratolysis is caused by Corynebacterium or Kytococcus bacteria thriving in moist, sweaty environments and responds well to topical benzoyl peroxide or clindamycin combined with moisture-wicking footwear and foot hygiene.
📋 Dr. Tom Biernacki, DPM, FACFAS answers:
Pitted keratolysis is caused by Corynebacterium bacteria thriving in moist, sweaty feet — not a fungus. It responds rapidly to topical antibiotics: erythromycin 2% or clindamycin 1% solution applied twice daily for 3–4 weeks clears most cases. Equally important: moisture control. Use antiperspirant sprays on the feet, change socks mid-day, wear moisture-wicking socks and breathable shoes. If topical antibiotics fail, oral erythromycin works well. Over-the-counter antifungals do nothing because this is bacterial, not fungal.
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.