
Quick answer: A cortisone shot in the foot delivers a corticosteroid directly into inflamed tissue — most commonly for plantar fasciitis, neuromas, or joint pain. The local anesthetic provides immediate relief; the steroid takes 3–14 days to reach peak effect. Risks include fat pad atrophy, blood sugar spikes in diabetics, and tendon weakening with repeated injections.

If your podiatrist has recommended a cortisone injection for foot pain, you probably have a dozen questions: Will it hurt? How fast will it work? Are there risks? How many can I get? Having performed thousands of these injections at Balance Foot & Ankle, I want to give you honest, detailed answers to all of them.
What Is a Cortisone Shot in the Foot?
Medically reviewed by Dr. Tom Biernacki, DPM

Board-certified podiatric surgeon | Balance Foot & Ankle | Last reviewed: May 2026
A cortisone injection — also called a corticosteroid injection — delivers a synthetic steroid directly into an inflamed structure in the foot or ankle. The most commonly injected corticosteroids are triamcinolone (Kenalog) and methylprednisolone (Depo-Medrol), usually combined with a local anesthetic like lidocaine for immediate pain relief. The steroid itself reduces prostaglandin synthesis and inflammatory cytokine activity, calming the inflammatory cascade that causes pain and swelling. In our practice, the most common targets are the plantar fascia (plantar fasciitis), first metatarsophalangeal joint (hallux limitus/rigidus, gout), Morton’s neuroma perineural tissue, peroneal tendon sheath, and the retrocalcaneal bursa.
What to Expect During the Injection
Most patients are surprised by how quick the procedure is — typically under five minutes. After cleaning the skin with betadine, we inject a small amount of local anesthetic into the superficial tissue, which stings briefly. Once the area is numb, the steroid is delivered precisely into the target structure. For deeper injections (joint spaces, perineural tissue), we may use ultrasound guidance to ensure accuracy and reduce the risk of tendon or fat pad damage. You’ll feel pressure but minimal pain once numb.
Key takeaway: Most patients rate the cortisone injection itself as a 2–3 out of 10 on a pain scale once the local anesthetic takes effect. The anticipation is almost always worse than the procedure.
How Long Does a Cortisone Shot Take to Work?
There are actually two phases of relief. The local anesthetic provides immediate relief for 2–6 hours — this is why some patients walk out of the office thinking the injection has already cured them. Then, as the anesthetic wears off, the original pain often returns and can temporarily feel worse for 24–48 hours (a normal “cortisone flare”). The actual steroid takes 3–5 days to begin working and typically reaches peak effect by 7–14 days. Relief can last anywhere from 4–6 weeks to 6 months depending on the diagnosis and injection site.
Risks and Side Effects
Cortisone injections are very safe when performed correctly, but there are real risks every patient deserves to understand before consenting to the procedure.
- Plantar fat pad atrophy: The most feared complication for heel injections — the protective fat pad under the heel thins with repeated steroid exposure, causing permanent increased pressure on the calcaneus. We limit plantar fascia injections to 2 per year for this reason.
- Plantar fascia rupture: Repeated cortisone weakens collagen fibers; injection directly into the fascia (rather than adjacent to it) increases rupture risk. We use ultrasound guidance to avoid intratendinous injection.
- Tendon weakening: Similar to fascia — injections into or adjacent to tendons (Achilles, peroneal) carry a rupture risk and are used very judiciously.
- Skin depigmentation or dimpling: Superficially placed steroid can depigment the overlying skin or cause a visible subcutaneous depression, more common in darker skin tones.
- Blood sugar spike: In diabetic patients, cortisone injections cause a transient 24–72 hour blood glucose elevation — typically 30–50 mg/dL above baseline. Monitor closely and alert your endocrinologist if you are on insulin.
- Infection: Rare (<1 in 10,000) but serious — single-use steroid vials and strict sterile technique minimize this risk.
⚠️ When to call your doctor after a cortisone injection:
- Increasing redness, warmth, and swelling 48+ hours after injection (possible infection)
- Sudden severe pain with a pop after returning to activity (possible tendon/fascia rupture)
- Diabetics: blood sugar elevation persisting more than 72 hours
- Skin color changes at the injection site
How Many Cortisone Shots Can You Get?
There is no universal maximum, but most evidence-based guidelines recommend no more than 3 injections per year at any single site, with at least 6 weeks between injections. For plantar fasciitis specifically, we limit to 2 per year due to fat pad atrophy risk. If a patient needs more than 2–3 injections to control a problem, that’s usually a signal that a more definitive intervention — custom orthotics, physical therapy, or surgery — needs to be reconsidered.
The Most Common Mistake We See
The most common mistake is using cortisone injections as a standalone treatment rather than a bridge to definitive care. Cortisone reduces inflammation — it doesn’t fix the underlying biomechanical cause of plantar fasciitis, neuroma, or joint arthritis. Patients who get an injection, feel 80% better, and then skip their stretching or orthotic program are back in our office 3–4 months later with the same problem. The injection buys you a window of low pain to do the rehabilitation work that actually produces lasting change.
Dr. Tom’s Picks: Post-Injection Support
For the 24-48 hour post-injection soreness (cortisone flare). Natural arnica formula — apply to injection area. Safe alongside corticosteroids topically.
View on Amazon →
After cortisone injection for plantar fasciitis or heel pain, proper arch support prevents re-aggravation. Maintain insole use for 6 weeks post-injection.
View on Amazon →
As an Amazon Associate I earn from qualifying purchases. As a Foundation Wellness partner I may also earn commission. Recommendations based on clinical experience.
⚠️ When to See a Podiatrist Before Considering Cortisone
- You feel relief that wears off in under 2 weeks repeatedly — this pattern suggests the underlying structural problem needs to be addressed, not just the inflammation.
- You’ve already had 3+ cortisone shots in the same area — each additional injection increases your risk of fat pad atrophy and tendon rupture.
- You’re a diabetic and haven’t checked your glucose in 24 hours — cortisone causes predictable blood sugar spikes that require monitoring for 3–5 days post-injection.
- The injection site becomes hot, red, or swollen 48+ hours after the shot — this is the classic presentation of post-injection infection (rare but serious) and requires urgent evaluation.
- You have pain waking you from sleep — night pain that’s unrelenting is a red flag for bone pathology or systemic disease that cortisone will not address.
Frequently Asked Questions
How long does a cortisone shot last in the foot?
Relief typically lasts 4–6 weeks for acute inflammatory conditions and 3–6 months for more chronic conditions when combined with corrective measures like orthotics and stretching. Some patients get relief for a year or longer.
Can I walk after a cortisone shot in my foot?
Yes — walking immediately after is fine for most injections. Avoid high-impact activity (running, jumping) for 48 hours to let the steroid settle and to reduce flare risk. You may be sore for 1–2 days while the anesthetic wears off.
Is cortisone the same as a steroid injection?
Cortisone is a type of corticosteroid, which is a broad class of anti-inflammatory steroids. Podiatrists most commonly use triamcinolone or methylprednisolone — both are corticosteroids that work similarly to cortisone but with slightly different duration profiles.
Get Your Cortisone Shot at Balance Foot & Ankle
Board-certified podiatric surgeons. In-office cortisone, PRP, and advanced injection therapy. Same-week availability at Howell and Bloomfield Hills, MI.
The Bottom Line
Cortisone injections in the foot are a safe, effective tool for temporarily controlling inflammation in plantar fasciitis, joint arthritis, neuromas, and bursitis. They work best as part of a thorough treatment plan — not as a substitute for one. If you’re considering a cortisone injection or want to know if it’s the right option for your foot pain, we’d be happy to evaluate you at Balance Foot & Ankle in Howell or Bloomfield Hills.
Cortisone vs. PRP: Which Injection Is Right for You?
At Balance Foot & Ankle, we offer both corticosteroid injections and platelet-rich plasma (PRP) therapy. The right choice depends on your diagnosis, how long you’ve had symptoms, and what you’ve already tried.
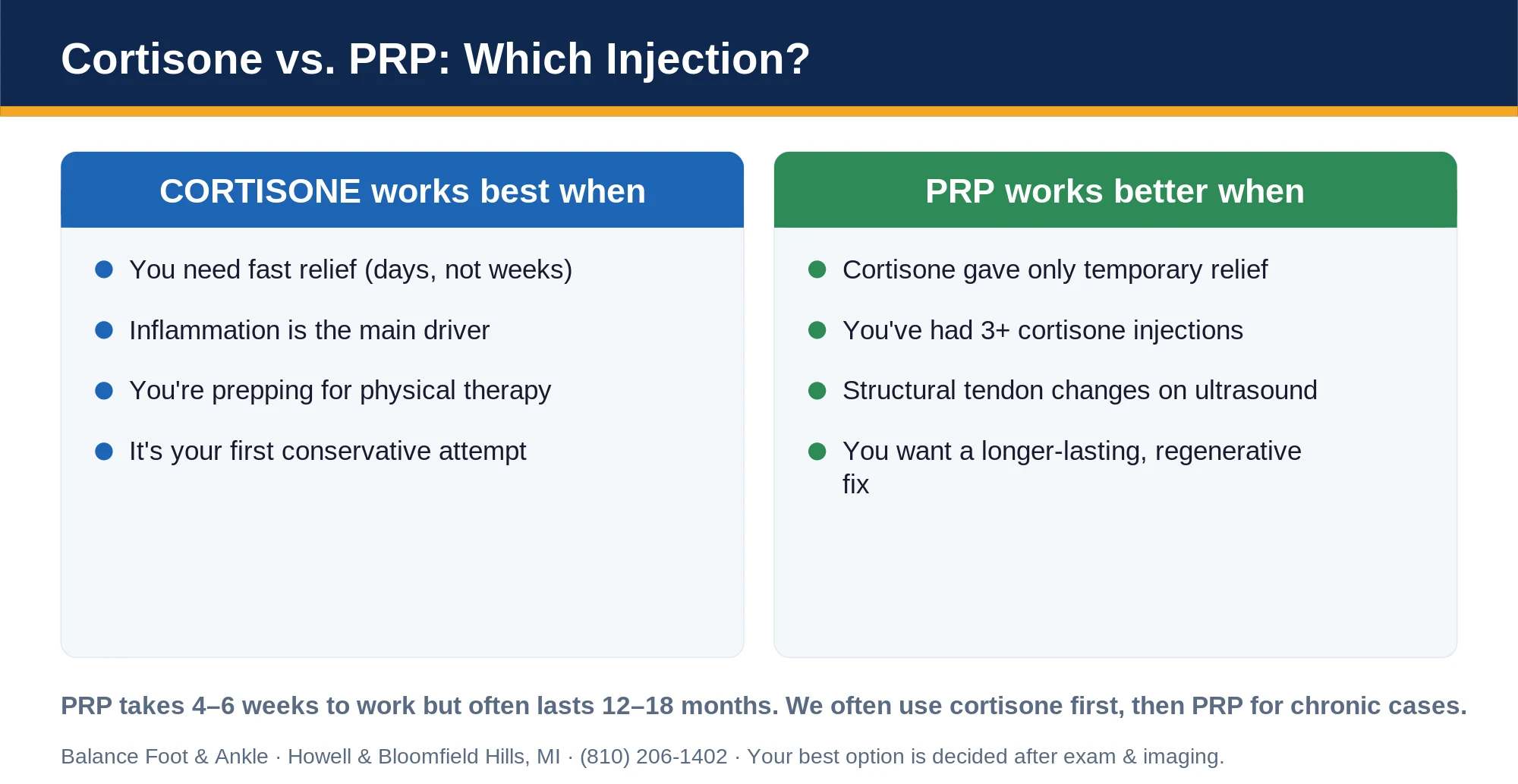
Cortisone works best when: You need fast pain relief (days, not weeks), inflammation is the primary driver (not structural damage), you’re preparing for physical therapy, or it’s your first conservative treatment attempt.
PRP works better when: Cortisone has provided only temporary relief, you’ve had more than three cortisone injections, structural tendon changes are present on ultrasound, or you want a longer-lasting regenerative approach. PRP takes 4–6 weeks to work but often lasts 12–18 months.
In our clinic, we frequently use cortisone first for acute flares, then transition to PRP for chronic conditions that have failed conservative care. Most patients with plantar fasciitis respond to one or two cortisone injections paired with stretching and orthotics — surgery is rarely needed.
Which Foot Conditions Respond Best to Cortisone?
Not every foot problem benefits equally from a cortisone injection. Here’s how we think about it at Balance Foot & Ankle:
- Plantar fasciitis — Excellent short-term response (80%+ of patients). Best used alongside stretching and arch support, not as a standalone fix.
- Morton’s neuroma — Very effective. Cortisone combined with a metatarsal pad often eliminates symptoms completely in mild-moderate cases.
- Bursitis — Responds quickly. Retrocalcaneal bursitis and intermetatarsal bursitis both respond well to targeted injection.
- Arthritis flares — Good for acute gout flares, big toe joint (hallux rigidus) flares, and ankle osteoarthritis flares. Not a long-term solution.
- Tarsal tunnel syndrome — Moderate response. Useful when nerve compression is partly from surrounding inflammation.
- Tendinitis — Use with caution. Cortisone near tendons (especially Achilles) carries rupture risk. We typically avoid direct tendon injections and inject the surrounding bursa instead.
Cost, Insurance & What to Expect at Your Appointment
Most insurance plans — including Blue Cross Blue Shield, Aetna, Cigna, United Healthcare, and Medicare — cover cortisone injections when medically indicated with a documented diagnosis. Prior authorization is rarely required for a first injection.
At Balance Foot & Ankle, the entire injection appointment typically takes 15–20 minutes. We start with a brief exam to confirm the target site, apply a topical numbing spray, and perform the injection under palpation guidance. Ultrasound guidance is available for complex cases. Most patients drive themselves home.
What to bring: Insurance card, photo ID, list of current medications (blood thinners require a brief hold), and any relevant imaging (X-rays or MRI). Call ahead if you take anticoagulants — we may need to coordinate with your prescribing physician.
Recovery Timeline: Day by Day After Your Injection
Knowing what to expect after a cortisone shot prevents unnecessary worry and helps you optimize recovery:
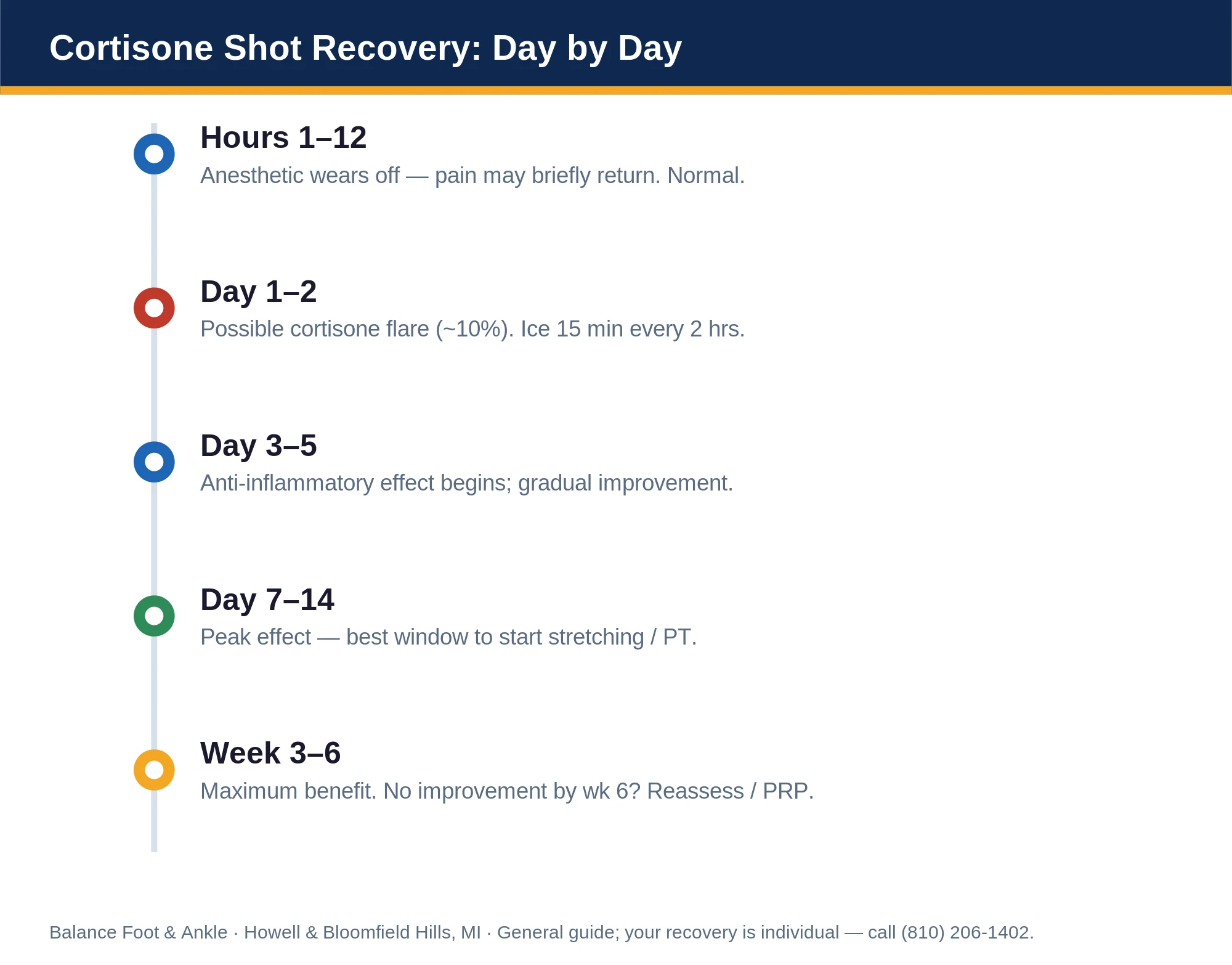
- Hours 1–12: The local anesthetic wears off. Some patients feel their pain return — this is normal and temporary.
- Day 1–2 (cortisone flare): About 10% of patients experience increased soreness. Ice 15 minutes every 2 hours. Avoid prolonged standing.
- Day 3–5: Anti-inflammatory effect begins. Most patients notice gradual improvement starting here.
- Day 7–14: Peak anti-inflammatory effect. This is the window to begin stretching and physical therapy for best results.
- Week 3–6: Maximum benefit achieved. If no improvement by week 6, reassess with imaging and discuss PRP or other options.
Activity guidelines: Light walking is fine immediately. Avoid high-impact activities (running, jumping) for 72 hours. Return to normal activity when pain allows — usually 3–5 days for most patients.
Post-Injection Recovery Essentials
Affiliate disclosure: As an Amazon Associate, Balance Foot & Ankle earns from qualifying purchases.
Apply for 10-15 min after injection to reduce swelling. Use for the first 24 hours.
Light compression helps reduce post-injection swelling and promotes circulation.
In our clinic, we always pair cortisone injections with a rehab protocol — stretching exercises, orthotic recommendations, and a follow-up at 4–6 weeks. An injection without a plan is only half the treatment.
Post-Injection Recovery Kit
Five items we recommend patients keep on hand for the first 48-72 hours after a cortisone injection in the foot. Ice + elevation + offloading + topical NSAID is the standard stack â these are the specific products we use in clinic.

Elasto-Gel Foot & Ankle Ice Pack
Ice for 15-20 minutes every 2 hours during the first 48-72 hours after a cortisone injection. A foot-shaped gel pack contours around the injection site (1st MTP, midfoot, heel) far better than a bag of cubes â and reusable for tendinopathy flares later.

Voltaren Arthritis Pain Gel (150g)
Topical diclofenac applied around (not on) the injection site adds local anti-inflammatory effect during the cortisone “wash-in” window. The 150g tube lasts a typical post-injection course. Avoid if you’re already on a high-dose oral NSAID â discuss with your podiatrist.

Darco OrthoWedge Post-Op Shoe
If your injection was in the 1st MTP joint or forefoot, an OrthoWedge takes load off the area for 48-72 hours while the cortisone settles. Most patients only need it for the first day or two â but having one in the closet for the next flare is worth $30.

Bauerfeind MalleoTrain Ankle Support
Gentle graduated compression for the first 48-72 hours reduces post-injection swelling and gives mild proprioceptive support if you’re walking on the foot. Easy to slip on under a sock. Remove for sleep and during icing.

Cushy Form Leg Elevation Pillow
Elevation above heart level overnight is the single highest-impact thing you can do for post-injection swelling. A wedge pillow keeps the foot at the right angle without sliding off a stack of regular pillows. Use for the first 2-3 nights post-injection.
Sources
- Monto RR. Platelet-rich plasma efficacy versus corticosteroid injection treatment for chronic severe plantar fasciitis. Foot Ankle Int. 2014.
- McMillan AM et al. Ultrasound-guided corticosteroid injection for plantar fasciitis. J Foot Ankle Res. 2012.
- Nichols AW. Complications associated with the use of corticosteroids in the treatment of athletic injuries. Clin J Sport Med. 2005.
Ready to Get Relief?
Same-day appointments available in Howell & Bloomfield Hills, MI
4.9★ | 1,123 Reviews | 3,000+ Surgeries
Or call: (810) 206-1402
In-Office Treatment at Balance Foot & Ankle
When home care and the right footwear aren’t enough for cortisone injection questions or foot & ankle pain, our team at Balance Foot & Ankle provides advanced evaluation and treatment at our Howell and Bloomfield Hills locations. Same-day appointments are available for acute and chronic conditions.
Same-day appointments available. (810) 206-1402
Learn about our cortisone injection therapy → | Book online →
Our podiatrists treat the underlying cause, not just the symptom. Same-week appointments at our Howell and Bloomfield Hills, Michigan offices.
Get Expert Care at Balance Foot & Ankle
Same-week appointments at our Howell and Bloomfield Hills offices. Board-certified podiatric surgeons. Most insurance accepted.
Same-Week Appointments in Howell & Bloomfield Hills
Three board-certified podiatric surgeons. 1,123+ five-star reviews. Most insurance accepted.
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.