
Ready to be seen? Book a real appointment time online, 24/7 — Howell or Bloomfield Township. Same-week openings are usually available.
Podiatrist’s Answer
To remove a foot corn at home: soften the area with warm water for 10–15 minutes, then gently file with a pumice stone. Never cut a corn with a blade — this risks infection. For painful or recurring corns, in-office removal under local anesthesia is safe, permanent, and takes under 20 minutes.
— Dr. Tom Biernacki, DPM, Board-Certified Podiatric Surgeon, Balance Foot & Ankle
Medically reviewed by Dr. Tom Biernacki, DPM
Board-certified podiatric surgeon | Balance Foot & Ankle
Last reviewed: May 2026
The most important step with a corn is finding what keeps pressing on that spot — a bony bump, a tight shoe, or a toe that rubs — because a corn shaved without relieving the pressure simply grows back. It also helps to confirm it’s a corn and not a plantar wart or callus, which are managed differently. We treat this at our Howell and Bloomfield Township offices. Call (810) 206-1402 or book a corn removal visit online.
If you have tried pumice stones, corn pads, and blade kits from the drugstore and the corn keeps coming back — you are not doing anything wrong. You are treating the symptom instead of the cause. In our clinic, we see patients who have been battling the same corn for years because they have been removing the thickened skin without addressing the underlying pressure that rebuilds it every few weeks.
This guide explains what foot corns actually are, how to tell them apart from calluses and warts (the three are often confused), what works at home, when to come in, and what we actually do during professional corn removal at Balance Foot & Ankle.
Quick answer: The safest way to remove a foot corn at home is to soak the foot in warm water for 10–15 minutes, gently reduce the thickened skin with a pumice stone, moisturize with a urea-based cream, and remove the pressure that caused it — roomier shoes or a cushioned pad. Never cut a corn with a razor, and skip medicated acid pads if you have diabetes or poor circulation.
What Is a Foot Corn?
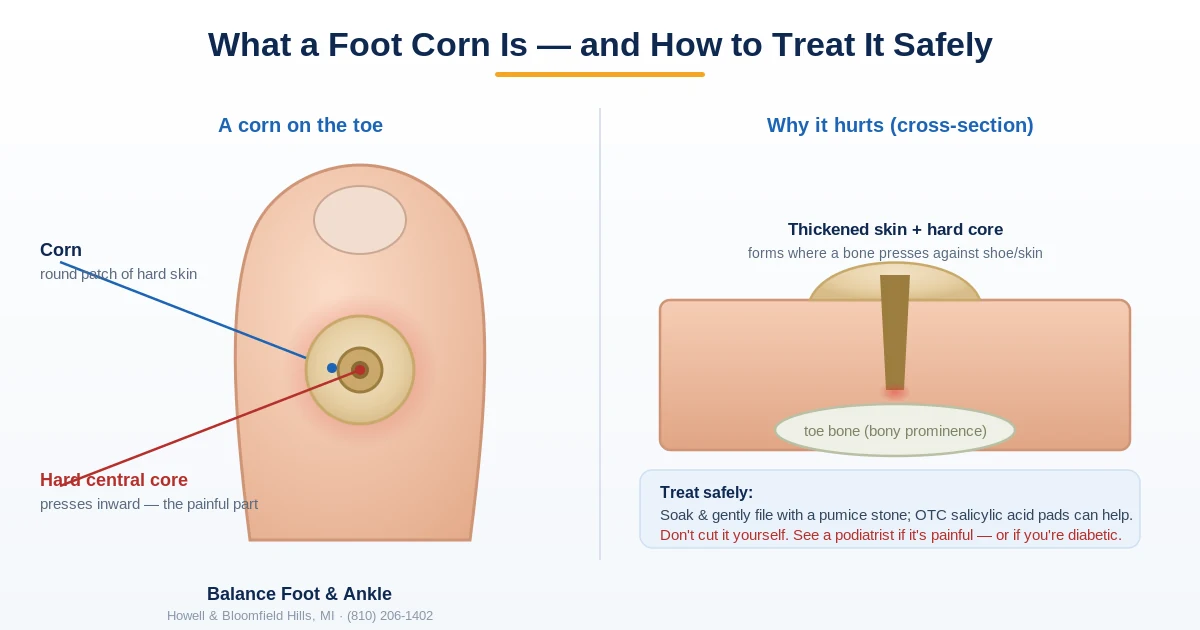
A foot corn is a concentrated, cone-shaped thickening of the outer skin layer (stratum corneum) that forms in response to repeated friction or pressure. Unlike a callus — which is a diffuse, flat area of thickened skin — a corn has a hard central core called the nucleus that points inward toward deeper tissue. This core is what creates the sharp, stabbing pain when you press on it or walk on it: the nucleus acts like a pebble embedded in your foot, concentrating force on the sensitive tissue beneath.
There are three main types. Hard corns (heloma durum) are the most common — small, firm, yellowish-white bumps that appear on the tops or sides of toes, or on the sole over a bony prominence. Soft corns (heloma molle) form between the toes, particularly between the fourth and fifth toes, where skin stays moist; they have a rubbery, whitish texture and are often misidentified as blisters or fungal infection. Seed corns (heloma miliare) are tiny, painless clusters of multiple small corns, usually on the heel or ball of the foot, often mistaken for plantar warts.
Key takeaway: The nucleus — the hard central core — is what makes corns painful. Removing the overlying skin without addressing the nucleus and the underlying pressure means the corn will regrow, typically within 4-8 weeks.
Corn vs. Callus vs. Plantar Wart: How to Tell the Difference

This is the most common diagnostic question we get, and it matters because the treatments are completely different. Treating a wart with salicylic acid corn pads can temporarily suppress it while the virus continues to spread. Treating a corn as a wart with aggressive freezing causes unnecessary pain and tissue damage.
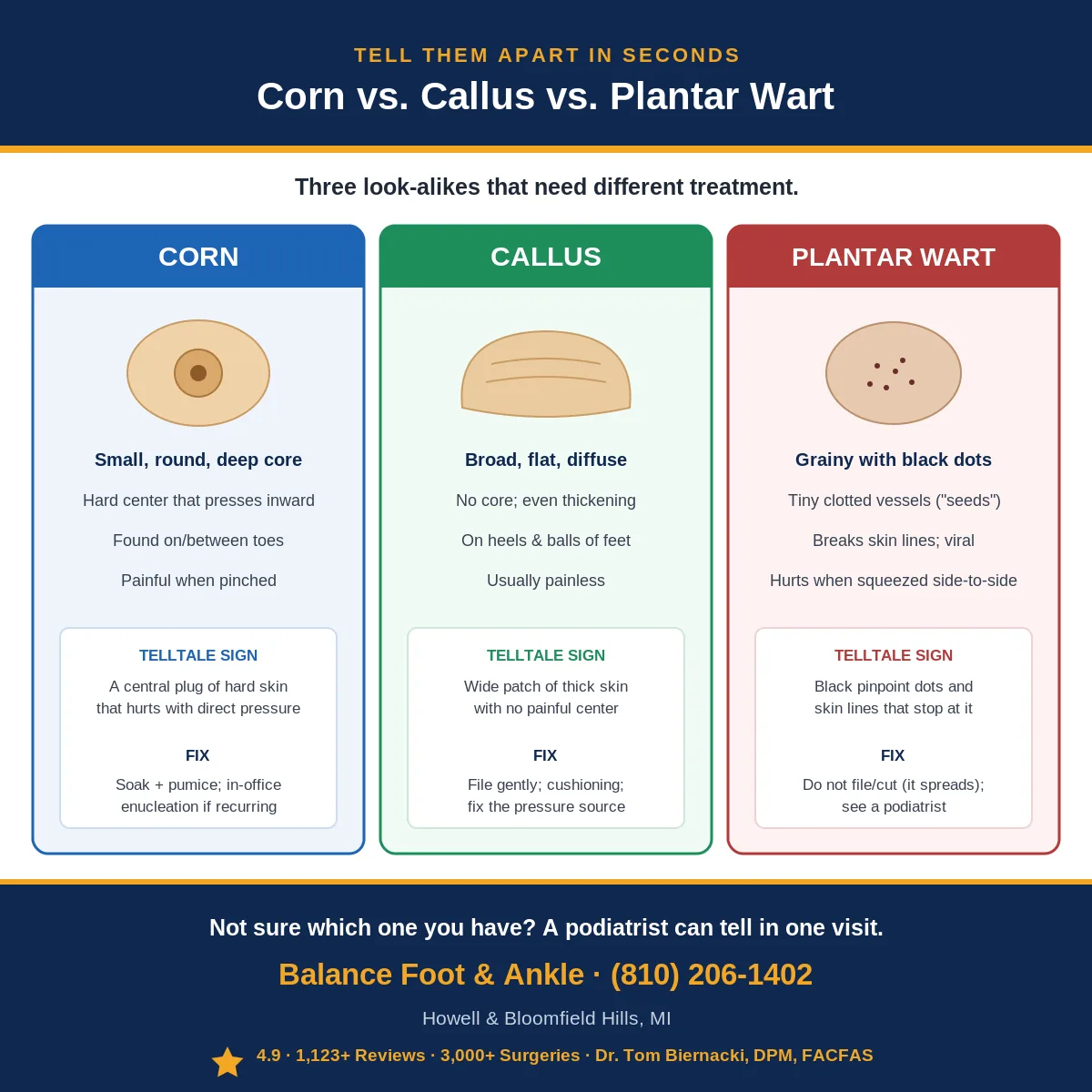
Corn: Located over a bony prominence or pressure point. Has a distinct, hard nucleus at the center. Skin lines (dermatoglyphics) run through the corn. Painful with direct downward pressure. No black dots or visible blood vessels.
Callus: Larger, flat, spread over a broad area. No central nucleus. Less painful or painless. Usually on the heel, ball of foot, or toe pads. Skin lines run through without interruption.
Plantar wart (verruca plantaris): Caused by HPV. Can appear anywhere on the plantar surface, not just over bony prominences. Skin lines are interrupted — they go around the wart rather than through it. Pinch the lesion side-to-side: warts hurt most with pinching, corns hurt most with direct downward pressure. May show small black dots (thrombosed capillaries). Multiple warts cluster together (mosaic pattern).
Key takeaway: The pinch test: squeeze the lesion side-to-side. Hurts most with pinching = suspect wart. Hurts most with direct downward pressure = suspect corn.
Side-by-Side Comparison: Corn, Callus or Wart
| Feature | Corn | Callus | Plantar wart |
|---|---|---|---|
| Where it forms | Over a bony prominence or pressure point | Broad weight-bearing areas (heel, ball of foot) | Anywhere on the sole — not just pressure points |
| Central core | Hard central nucleus | None | No core; may show tiny black dots |
| Skin lines | Run through the lesion | Run through, uninterrupted | Interrupted — lines go around it |
| What hurts most | Direct downward pressure | Mild or painless | Pinching side-to-side |
| Cause | Friction / pressure | Friction / pressure | HPV virus (contagious) |
What Causes Foot Corns?
The mechanism is straightforward: repetitive friction or pressure on a specific point of skin triggers a protective response. Skin cells in that area proliferate faster, producing more keratin. Over time, the thickened skin consolidates into a corn with its central nucleus.
The most common causes we identify include: ill-fitting footwear (the leading cause — shoes too narrow, too shallow, or with prominent seams; high heels that force weight onto the forefoot); bony prominences due to hammertoe, bunion, or structural deformities where the toe contacts the shoe; gait abnormalities causing uneven weight distribution; going barefoot frequently on hard surfaces; and fat pad atrophy (the natural cushioning under the forefoot thins after age 40).
Soft corns between the toes form when two adjacent bony prominences press against each other — common when the fourth toe has a lateral condyle (bony bump) contacting the fifth toe. Moist, enclosed footwear accelerates skin maceration and increases friction injury.
Home Treatment for Foot Corns: What Actually Works

For mild, non-painful corns in people without diabetes, poor circulation, or neuropathy, home treatment is reasonable. The goal is managing thickness while simultaneously reducing the pressure causing the corn.
Salicylic acid is the only OTC treatment with genuine evidence. It works as a keratolytic — it chemically dissolves keratin, the primary component of the corn. Available as pads (40% concentration) and liquids (17%). Protocol: soak the foot 5-10 minutes, dry thoroughly, apply the pad to the corn only (not surrounding skin), leave 24-48 hours, remove, use a pumice stone on the softened white tissue. Repeat weekly. Expect 4-8 weeks for significant improvement.
Pressure-relief padding is equally important and often overlooked. Donut-shaped felt pads placed around the corn redistribute pressure away from the nucleus. This reduces pain immediately and slows regrowth by reducing the mechanical stimulus. Without addressing the pressure, any removal is temporary.
Urea cream (10-25% concentration) applied nightly prevents the corn from becoming excessively hard. Urea is also keratolytic at higher concentrations — it both softens and slowly dissolves thickened tissue over time.
Key takeaway: Salicylic acid + donut padding + urea moisturizer works significantly better than any single approach. Salicylic acid removes existing tissue; padding prevents pressure-driven regrowth; urea maintains pliability.
Corn Treatment at a Glance
| Approach | Best for | What to expect |
|---|---|---|
| Salicylic acid (40% pad / 17% liquid) | Mild corns; no diabetes, neuropathy, or poor circulation | Weekly; 4–8 weeks for clear improvement |
| Donut pressure-relief padding | Immediate pain relief & slowing regrowth | Redistributes pressure off the nucleus |
| Urea cream (10–25%) | Keeping skin soft and preventing rebuild | Apply nightly; softens over time |
| Professional debridement | Painful or recurring corns; soft corns between toes | 10–20 min, painless, immediate relief |
| Fixing the cause (orthotics, footwear, surgery) | Corns that keep returning from a deformity | 6–12 months relief; long-term with surgical correction |
What Not to Do: Home Corn Removal Mistakes
The most dangerous mistake is using blade-type corn removal tools at home. While professionals use similar instruments, home use carries significant infection risk. The skin beneath a corn can have microscopic breaks, and cutting too deeply causes bleeding, introduces bacteria, and can lead to serious soft tissue infections — especially dangerous in people with diabetes or peripheral vascular disease.
Other mistakes: applying salicylic acid to soft corns between the toes (the acid plus the moist environment creates perfect conditions for fungal or bacterial infection); using corn pads on broken skin; and attempting to “dig out” the nucleus with a nail file (this does not work and causes tissue damage).
⚠️ Do NOT attempt home corn removal if you have
- Diabetes (any type) — even small wounds on the feet can become limb-threatening
- Peripheral arterial disease or poor circulation — healing is impaired and infection risk is elevated
- Peripheral neuropathy — you may not feel if you have cut too deep
- A soft corn between the toes — professional treatment is safer here
- Redness, warmth, swelling, or drainage around the corn — this needs immediate medical evaluation
- Difficulty seeing the corn clearly due to mobility issues — unsafe instrument use is a major infection risk
Professional Foot Corn Removal: What Happens at the Podiatrist

When a patient comes to our clinic for corn removal, the procedure is straightforward, typically takes 10-20 minutes, and provides immediate pain relief. Here is what to expect from a professional corn removal appointment.
Assessment first: We examine the corn type, location, size, depth, and the structural cause. Is there a hammertoe causing the toe to rub the shoe? A bunion redirecting pressure? An equinus contracture increasing forefoot loading? The treatment plan depends on addressing the cause.
Debridement: Using a sterile scalpel or curette, we carefully pare down the corn layer by layer until healthy skin is reached and the nucleus is eliminated. This is painless when done correctly — the thickened tissue has no nerve endings, and we stop well before reaching sensitive tissue. Patients are consistently surprised at how painless this procedure is after tolerating the corn pain for months.
Addressing the cause: Depending on the structural cause, we may pad the foot with felt or silicone to redistribute pressure, prescribe custom orthotics, recommend footwear changes, or discuss surgical correction of hammertoe or bunion deformities for cases where the bony prominence will never resolve with conservative care.
For soft corns between toes: Treatment involves debridement plus a silicone toe spacer worn between the affected toes. In recurrent cases, a condylectomy — removing the bony bump on the side of the toe — permanently eliminates the structural cause. When the culprit is a bony bump on the outer edge of the foot, see our guide to a protruding bone on the outside of the foot.
Can You Remove a Corn Overnight?
Honestly, no — and any product promising it isn’t being straight with you. A corn is a thick plug of hardened, dead skin your body built up over weeks in response to repeated pressure or friction, so there’s no safe way to make it disappear by morning. What you can do is start that same night: soak your foot in warm water for 10–15 minutes and gently smooth the top with a pumice stone or foot file. Repeat nightly and a small corn often flattens noticeably within a few days. A medicated salicylic-acid corn pad can speed things up by dissolving the dead skin over several days — but skip the pads if you have diabetes, poor circulation, or numbness, because they can damage healthy skin and open a wound. The fastest safe route to relief is in-office removal: a podiatrist can pare down a painful corn under local anesthesia in under 20 minutes. Whichever path you choose, the corn will keep returning until you relieve the pressure causing it — better-fitting footwear, padding, or an orthotic is what actually keeps it gone. Which of those three you need depends on what is actually driving the pressure, and that is a question about the joint underneath rather than the skin on top. Book a corn assessment online.
How Long Does It Take for a Corn to Go Away?
This depends heavily on whether you address the cause. After professional debridement with no mechanical correction, most corns regrow to painful levels within 4-12 weeks. With appropriate pressure offloading via padding or orthotics, recurrence is dramatically slower — many patients go 6-12 months between treatments. With surgical correction of the underlying deformity, recurrence rate is very low.
Home salicylic acid treatment requires patience: 4-6 weeks for significant improvement, up to 8-12 weeks for a well-established corn. The corn will look worse before better — salicylic acid turns the treated area white and soft before tissue sloughs off.
Key takeaway: Debridement alone = temporary. Debridement + pressure offloading = 6-12 months relief. Surgical correction of the bony prominence = long-term resolution.
Corn Prevention: Stopping Them from Coming Back
The most important preventive measure is addressing footwear fit. Shoes need enough depth in the toe box so the toes do not press against the shoe ceiling — the most common cause of dorsal (top-of-toe) corns. Toe box width matters equally: narrow boxes compress the forefoot, creating inter-toe pressure leading to soft corns and lateral toe corns. Have your foot professionally measured — most people are wearing shoes in the wrong width.
For people prone to corns, regular mechanical debridement — at home with a pumice stone on soaked skin, or professionally at 8-12 week intervals — prevents individual lesions from growing large enough to become painful. Think of it as maintenance, not a cure. If you have a fixed structural deformity, custom orthotics redistribute plantar pressure well, but dorsal toe corns from the toe rubbing the shoe ceiling require either better-fitting shoes or surgical correction.
Footwear & Orthotics That Prevent Corns
Most corns come from repeated pressure or friction inside shoes. To stop them returning, see our podiatrist-recommended shoes with roomier toe boxes, plus recommended orthotics to redistribute pressure. If a corn keeps coming back or hurts, book an evaluation.
In-Office Corn Removal at Balance Foot & Ankle
If a corn is too painful to treat at home, keeps coming back, or is between the toes where home care is difficult, professional enucleation is the safest option. At Balance Foot & Ankle, Dr. Tom Biernacki DPM provides in-office corn removal for patients in Howell and Bloomfield Township, MI. Recurring corns caused by structural deformity may also benefit from hammertoe treatment to fix the root cause.
Frequently Asked Questions
Does it hurt to have a corn removed by a podiatrist?
Professional corn debridement is almost always painless. The thickened keratinized tissue has minimal nerve density, and a skilled podiatrist removes the corn layer by layer without reaching sensitive live tissue. Most patients are surprised at how comfortable the procedure is compared to how much the corn hurt during daily walking. Local anesthesia is generally not required for standard debridement.
Can I remove a foot corn myself?
You can safely use salicylic acid pads and donut-shaped pressure-relief cushions for mild corns if you do not have diabetes, neuropathy, or poor circulation. Do not use blade-type corn razors at home — these create infection risk. For soft corns between toes, or any corn in a person with diabetes or vascular disease, always see a podiatrist.
Why does my corn keep coming back?
Corns return because the mechanical cause — friction or pressure from a bony prominence contacting footwear — has not been addressed. Removing the corn tissue only eliminates the lesion temporarily; the skin rebuilds under continued pressure. Long-term resolution requires addressing footwear fit, using pressure-redistribution padding or orthotics, or (for structural deformities like hammertoes) corrective surgery.
Are corn removal pads safe?
Medicated corn pads containing 40% salicylic acid are safe for adults without diabetes, neuropathy, or skin conditions when applied to intact, healthy skin. Apply to the corn only, not surrounding skin. Never use between the toes or on broken skin. If you have any vascular or nerve condition in your feet, skip OTC treatments and see a podiatrist.
How do I know if my corn is infected?
Signs of infection include: increasing redness spreading beyond the corn, warmth, swelling, pus or cloudy drainage, fever, red streaking up the foot or leg (lymphangitis), or pain that is worsening rather than stable. Any of these findings requires prompt medical evaluation — do not attempt home treatment of an infected corn.
The Bottom Line
Foot corn removal is effective, but its effectiveness depends on matching treatment to cause. Salicylic acid and donut padding manage mild corns at home. Professional debridement provides immediate relief — patients walk out with dramatically less pain than when they walked in. But lasting results require addressing the underlying mechanical problem: the footwear, gait pattern, or bony deformity driving the corn.
If you have a corn that keeps coming back, a soft corn between toes that will not respond to treatment, or any concern about corns in the context of diabetes or circulation issues, please come in. Same-day appointments are available at our Howell and Bloomfield Township locations.
Ready to Remove That Corn for Good?
Same-day appointments available in Howell & Bloomfield Township, MI
4.9★ | 1,123 Reviews | 3,000+ Surgeries Performed
Or call: (810) 206-1402
Sources
1. Farndon LJ, Vernon W, Walters SJ, et al. The effectiveness of salicylic acid plasters compared with usual scalpel debridement of corns: a randomised controlled trial. J Foot Ankle Res. 2013;6(1):40.
2. Vlahovic TC, Dunn SP, Blume P. The use of a topical 40% urea compound for the treatment of hyperkeratotic conditions. J Am Podiatr Med Assoc. 2010;100(6):475-479.
3. Springett K, Whiting M, Marriott C. Epidemiology of plantar forefoot corns and the effect of off-loading. Foot. 2003;13(1):5-10.
4. Hashmi F, Richards BS, Forghany S, et al. The formation of plantar forefoot corns in older people: a qualitative study. J Foot Ankle Res. 2012;5(1):16.
5. Singh D, Bentley G, Trevino SG. Callosities, corns, and calluses. BMJ. 1996;312(7043):1403-1406.
Related guide: Corns and calluses often share the same cause. See our complete Corns & Calluses Treatment Guide — causes, prevention, and when podiatric debridement is the right choice.
Related skin-lesion guides
More on corns, calluses and foot-skin lesions:
Recurring corns can signal a deeper pressure problem — learn more in our foot & ankle conditions guide.
Painful corn that keeps coming back?
Corns return until the pressure causing them is fixed — and home removal is risky if you’re diabetic. In Michigan? our podiatrists remove them safely and stop the cycle. Same-week visits in Howell & Bloomfield Township, most insurance accepted.
📅 Book an Appointment 📞 (810) 206-1402★ 4.9 from 1,123+ Google reviews · Same-week visits · We verify your insurance free — most visits are just a copay.
Noticing yellow skin along with the corn? Thickened, callused skin often takes on a yellowish tone — but that is not the only cause. Here is a podiatrist’s rundown of why the bottoms of your feet can look yellow and when it is worth checking out.
Book an appointment with a podiatrist
A corn that keeps coming back is being caused by pressure somewhere, and taking it off at home without changing that pressure means it returns every few weeks. A podiatrist can pare it painlessly and find the cause. Balance Foot & Ankle sees patients at two offices — Howell in Livingston County, and Bloomfield Township in Oakland County.
Book online, 24/7: choose a real appointment time at Howell or Bloomfield Township. Prefer to speak with someone first? Call (810) 206-1402 or use the form below.
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.
More questions patients ask
How do you safely remove a corn from your foot at home?
Soak the area in warm water for 10–15 minutes to soften the skin, then gently file with a pumice stone. Apply a salicylic acid corn pad and keep pressure off the area with cushioned footwear. Never cut a corn yourself — this risks infection. See a podiatrist for safe, professional removal.
What is the difference between a corn and a callus?
A corn is a small, focused area of hard skin with a central core that presses on nerves, causing sharp pain. A callus is a broader, flatter area of thickened skin with no central core and is usually painless. Both are caused by friction and pressure from shoes or foot deformities.
When should I see a podiatrist for a corn?
See a podiatrist if your corn is very painful, becomes red or infected, keeps coming back despite home treatment, or if you have diabetes or poor circulation. A podiatrist can safely remove the corn and address the underlying cause, such as hammertoe or ill-fitting shoes.
How do you safely remove a corn from your foot?
Safe corn removal starts with eliminating pressure (wider shoes, padding). Salicylic acid patches (40%) soften the core over 1–2 weeks. A podiatrist can perform painless sharp debridement in one visit — the safest and fastest method.
Do corn removal pads really work?
Salicylic acid corn pads (Compound W, Dr. Scholl's) work for soft tissue corns if used consistently. They are NOT appropriate for diabetic patients or corns with a very deep core. Removing the pressure source is always step one.
Can you cut a corn off at home?
Never use a razor blade or scissors to cut a corn — risk of infection and nerve injury. Use only gentle pumice after softening with salicylic acid. Diabetic patients should never self-treat — any corn needs podiatric evaluation.
When should I see a podiatrist for a foot corn?
See a DPM if the corn is painful with walking, has returned after home treatment, or you are diabetic. Same-day appointments available at Balance Foot & Ankle — (810) 206-1402 — Howell & Bloomfield Township, MI.
How do you remove a corn from your foot at home?
Soak the foot in warm water for 10 minutes to soften the corn. Gently file with a pumice stone in one direction. Apply 40% salicylic acid corn pad and replace daily. Wear cushioned shoes with a wide toe box to prevent recurrence. Never cut corns yourself if you have diabetes or circulation problems.
What dissolves a foot corn fast?
Salicylic acid (40%) dissolves corns the fastest of OTC products. Apply daily for 7-10 days alongside daily filing. For stubborn corns, see a podiatrist for in-office sharp debridement, which provides immediate relief. Cryotherapy is also effective for resistant corns. Avoid over-the-counter cutting tools to prevent infection.
What causes corns on feet?
Corns form from chronic friction or pressure. Common causes include shoes that are too tight, hammertoes, bunion deformities, high-heeled shoes, gait abnormalities, and bony prominences. Without addressing the underlying mechanical cause, corns will return. A podiatrist evaluates for biomechanical contributors and may recommend orthotics or surgery.
When should you see a podiatrist for a corn?
See a podiatrist if you have diabetes or circulation problems, the corn is painful, recurs after home treatment, has signs of infection (redness, warmth, drainage), or limits walking. We provide painless sharp debridement, identify the mechanical cause, and prevent recurrence through footwear and orthotic correction.
What is the fastest way to remove a corn from your foot?
The fastest professional method is debridement by a podiatrist — the corn is trimmed with a sterile blade in minutes with no anesthesia needed. At-home salicylic acid (40% patches or liquid) softens the corn over 3–7 days but is slower. Never try to cut a corn yourself, as infection risk is significant.
Can you remove a foot corn at home?
Soft corns and small hard corns can be managed at home with 40% salicylic acid patches, pumice stone use after soaking, and proper shoe fit. However, diabetic patients and anyone with poor circulation should never attempt home corn removal — even minor skin breaks can lead to serious infections. See a podiatrist if it returns.
How long does it take for a foot corn to go away?
With consistent salicylic acid treatment, a small corn typically softens and resolves in 1–4 weeks. Larger or deeper corns (seed corns under callus) may take 4–8 weeks or require professional debridement. Corns will return if the underlying cause — pressure from shoe fit or foot mechanics — is not corrected.
Does insurance cover corn removal by a podiatrist?
Most insurance plans, including Medicare Part B, cover medically necessary corn removal when the corn causes pain or functional limitation and conservative home treatment has failed. A podiatrist visit for corn debridement is typically billed under routine foot care codes. Coverage for orthotics to prevent recurrence varies by plan.
Still have a question about coverage or cost? Book online and we will check your benefits before your visit: Book in Howell · Book in Bloomfield Township. Prefer to talk it through first? Call (810) 206-1402.