
Quick answer: A stone bruise is a deep, localized pain in the ball or heel of the foot that feels like stepping on a pebble — usually from impact, a hard object, or repetitive pressure. Most resolve with rest, cushioned shoes, and a metatarsal pad over a few weeks; severe or lasting pain should be checked to rule out a stress fracture or bruised fat pad.
Ready to be seen? Book a real appointment time online, 24/7 — Howell or Bloomfield Hills. Same-week openings are usually available.
Medically reviewed by Dr. Tom Biernacki, DPM
Board-certified podiatric surgeon | Balance Foot & Ankle
Last reviewed: May 2026
Almost everyone has experienced it: you step down and immediately feel like there is a stone or marble lodged under the ball of your foot — but when you check, there is nothing there. This “stone bruise” sensation is one of the most common forefoot complaints we see in our Howell and Bloomfield Hills clinics. The frustration is that it keeps coming back with every step, often for days or weeks. Understanding what is actually causing it determines whether rest and better shoes are all you need, or whether something more significant is going on.

- COMFORTABLE SUPPORT: 1/4 inch thick felt metatarsal pads provide gentle cushioning under the ball of the foot for daily wear
- VALUE PACK: Includes 6 pairs (12 pieces) to ensure long-lasting comfort and convenience
- ADHESIVE BACKING: Strong adhesive keeps the pad in place inside shoes or directly on the foot
- MADE IN THE USA: Proudly designed, cut, and manufactured in the United States
- EASY TO CUSTOMIZE: Can be trimmed with scissors for a better fit inside a variety of footwear

- ENGINEERED MESH
- Lining Textile
As an Amazon Associate, Balance Foot and Ankle earns from qualifying purchases. Product links are affiliate links and we may earn a commission at no extra cost to you. This does not influence our clinical recommendations. Last update on 2026-07-26 / Images from Amazon Product Advertising API
A “stone bruise” is not a single diagnosis — it is a symptom pointing to one of five underlying causes: metatarsal overload, fat pad atrophy, plantar plate injury, Morton’s neuroma, or sesamoid injury. Each requires a different treatment. Rest and cushioned shoes help short-term, but if forefoot pain keeps returning in the same spot, a podiatrist needs to identify the specific cause to fix it permanently.
What Is a Stone Bruise?
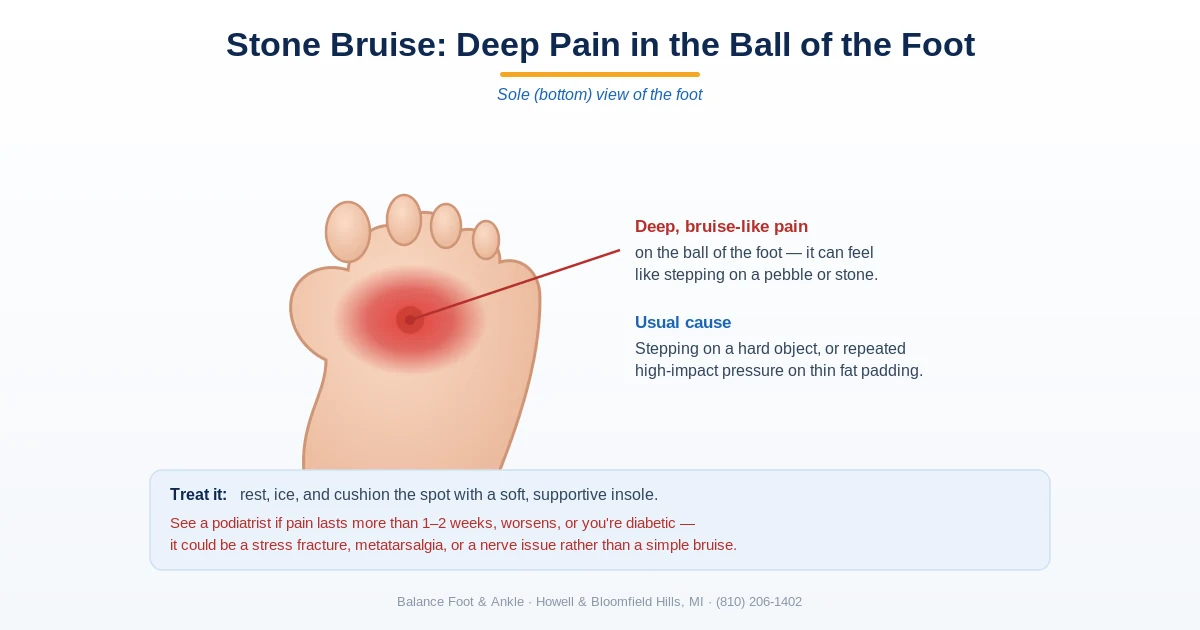
A “stone bruise” is not an official medical diagnosis — it is a descriptive term for pain under the forefoot or heel that replicates the feeling of walking on a pebble. The pain is typically sharp or aching, precisely localized under one or more metatarsal heads (the bony prominences at the ball of the foot), and is weight-bearing dependent — worse with every step on hard surfaces, better when off your feet.
In its most literal form, a stone bruise is a direct bone contusion of the plantar surface of a metatarsal head or the heel bone, caused by stepping hard on a sharp object — a stone, a hard Lego brick, an uneven surface. The periosteum (the sensitive membrane covering the bone) is bruised and inflamed. This type resolves in days to 2 weeks with rest and cushioning.
But in clinical practice, when a patient complains of a stone bruise that has persisted for weeks or keeps recurring, we are almost always dealing with one of the conditions below rather than a simple bone contusion.
Key takeaway: The term ‘stone bruise’ is a colloquial description, not a clinical diagnosis. It describes the sensation — walking on a pebble — caused by several underlying conditions, most commonly metatarsalgia (overloaded metatarsal heads), fat pad atrophy, or a genuine bone contusion from direct impact. Treating the symptom without identifying the cause leads to slow recovery and recurrence.
What a Stone Bruise Actually Looks Like
Most of the time it looks like nothing at all. Patients arrive certain that something must be visible on the sole, and in the large majority of cases the skin over the sore spot is completely normal: the same color and the same texture as the matching spot on the other foot. That surprises people, and it is the most common reason this injury gets waved off as nothing by someone who has taken a look at it.
The explanation is anatomical. The injured tissue sits deep, in the fat pad and the periosteum lying directly on bone, buried beneath a dense fibrous layer and some of the thickest skin on the body. Blood from a bruise down there has almost no route to the surface, so there is usually nothing to see even when the injury is entirely real.
Visible discoloration does happen, but generally only after a genuinely violent impact: a hard landing off a ladder, a dropped weight plate, a misjudged step off a curb at speed. When it appears it tends to appear late, often two to four days afterward, and it surfaces where gravity carries it rather than where it hurts. Expect it along the sides of the heel, in the web spaces between the toes, or spreading across the top of the foot. A bruise that emerges in one of those places while the pain stays underneath is behaving exactly as it should.
Two things are regularly mistaken for a visible stone bruise. The first is a callus, a firm yellowish patch of thickened skin that builds over a spot taking too much load. It is a marker of the pressure that caused the problem rather than evidence of the bruise itself. The second is a small dark dot, which is far more likely to be a plantar wart or a splinter that has sealed over than any kind of bleeding beneath the skin.
What is worth doing instead is mapping it. Sit down, cross the sore foot over the opposite knee, and press with the pad of one thumb, moving in small steps across the sole. A stone bruise maps as a tender area roughly the size of a coin, centered under a fat pad, and it goes quiet everywhere around that. Soreness that runs as a narrow band along the length of a bone, or that flares when you compress the foot from both sides, is a different problem and belongs in front of a clinician.
One practical note for anyone searching for pictures of this: photographs of the sole are close to useless here, because the information a clinician needs is not on the skin. What a podiatrist works from is where your thumb finds the tenderness, what you were doing when it started, and how it has behaved since. A clear account of those three things is worth more than any photograph.
Cause 1: Metatarsalgia — Overloaded Metatarsal Heads
Metatarsalgia is the most common cause of persistent stone bruise-like pain. It refers to pain and inflammation directly under the metatarsal heads — the five knuckle-like bones at the ball of the foot — due to excessive or abnormal loading. Under normal gait, the metatarsal heads share the forefoot load. When one or more metatarsal heads bear disproportionate pressure, the overlying tissue (plantar plate, joint capsule, periosteum) becomes chronically inflamed.
Common causes of metatarsal overloading: high-heeled shoes (which shift body weight forward onto the metatarsal heads), a longer-than-normal second or third metatarsal (transferring excess load to that bone), bunion deformity (offloading the first metatarsal and forcing more load onto the second), tight calf muscles (equinus contracture that forces more forefoot loading), and excessive mileage in runners with thin-soled shoes.
Treatment for metatarsalgia: metatarsal pad placed just behind (proximal to) the affected metatarsal head to redistribute load away from it, custom orthotic with appropriate metatarsal accommodation, rocker-bottom footwear modification, calf stretching program, and activity modification during the acute phase.
Cause 2: Plantar Fat Pad Atrophy
Under the metatarsal heads and heel, the foot is naturally cushioned by a specialized compartmentalized fat pad — a cellular structure of fat enclosed in fibrous chambers that is specifically engineered to absorb impact. This fat pad thins progressively with age, cumulative impact loading (marathon runners, prolonged barefoot walkers), and after repeated corticosteroid injections into the forefoot.
When the fat pad is depleted, the metatarsal heads become nearly unprotected on hard surfaces — each step transfers the full ground reaction force directly to the bone. Patients describe it as “walking on bones.” The pain is diffuse across the ball of the foot rather than localized to a single metatarsal head, and worsens dramatically on hard floors and in thin-soled shoes.
Key takeaway: Plantar fat pad atrophy is an underdiagnosed cause of stone bruise-like pain, especially in adults over 50. The fat pad that naturally cushions the metatarsal heads and heel thins with age, high cumulative impact, and prior corticosteroid injections — leaving the bony prominences unprotected. Custom orthotics with appropriate padding can simulate the missing fat pad and provide dramatic relief.
Treatment for fat pad atrophy: there is no way to regenerate the lost fat pad, but its function can be simulated. Cushioned custom orthotics with a softer durometer (hardness) forefoot material spread the load across the entire metatarsal region. Shoes with maximalist cushioning (thick EVA or polyurethane midsoles) reduce peak metatarsal pressures substantially. Autologous fat grafting (injecting fat harvested from elsewhere in the body into the plantar fat pad) is an emerging surgical option with promising early results for severe cases.
Cause 3: Plantar Plate Injury
The plantar plate is a thick, fibrocartilaginous ligament on the undersurface of each metatarsophalangeal joint (the joint where the toe meets the metatarsal). It is the primary restraint preventing the toe from dorsiflexing (bending upward) excessively. Repetitive hyperextension — common in runners at toe-off, in people who squat frequently, or in anyone who climbs stairs heavily — can create microtears in the plantar plate, a condition called plantar plate tear or predislocation syndrome.
A plantar plate tear produces pain specifically under the second or third metatarsophalangeal joint — identical in location to a stone bruise — along with a sense of instability in the toe and occasional toe drifting or crossing (the toe begins to deviate toward the adjacent toe when the plantar plate can no longer hold it in place). The “paper pull-out test” (a paper slip under the toe is difficult to pull out when the plantar plate is intact, and easy to pull out when torn) confirms plantar plate incompetence clinically. MRI or diagnostic ultrasound confirm tear extent.
Cause 4: Morton’s Neuroma
Morton’s neuroma (interdigital neuroma) primarily produces burning and numbness between the toes, but early or atypical cases can present simply as pain under the ball of the foot that feels like a stone bruise. The nerve thickening between the third and fourth metatarsal heads creates a sensation of a lump or pebble under the forefoot, particularly when the metatarsal heads are compressed by narrow footwear.
The distinguishing features: Mulder’s click (a palpable/audible click when compressing the forefoot while pressing on the interspace), pain or numbness shooting into the toes, and location specifically in the 3–4 intermetatarsal space rather than directly under a metatarsal head. Ultrasound confirms the neuroma and guides injection therapy.
Cause 5: Sesamoid Injury
The two sesamoid bones under the first metatarsal head are located exactly where a stone bruise at the medial forefoot would occur. Sesamoiditis (inflammation), a sesamoid stress fracture, or sesamoid avascular necrosis all produce pain in this precise location that is easily mistaken for a stone bruise. The key distinguishing feature: the pain is specifically under the great toe’s metatarsophalangeal joint (ball of foot, inner side), worst with big toe extension and pushing off, and may have a history of high-impact activities (ballet, running, jumping sports).
X-ray with a special sesamoid axial view evaluates for fracture and bipartite sesamoid. MRI or bone scan detects avascular necrosis or stress reaction not visible on plain X-ray. Treatment ranges from offloading padding and dancer’s pads to surgery (sesamoidectomy) for recalcitrant cases.
Key takeaway: The most important differential for a stone bruise that is not improving after 4 weeks: stress fracture of the metatarsal. A stress fracture also produces pain under the ball of the foot, but the tenderness is more precisely localized to a single metatarsal shaft and worsens over days to weeks of continued activity. X-ray (often negative early) and MRI confirm the diagnosis — do not miss a stress fracture by assuming it is metatarsalgia.
Where It Hurts: Heel, Ball of the Foot, or Arch
The five causes above are all forefoot problems, which reflects where most of these injuries actually land. But the same complaint, described in exactly the same words, means something different depending on which part of the sole it is coming from. Location is the fastest way to narrow it down, and it changes what belongs in the shoe.
Under the heel
The heel carries its own shock absorber, a chambered fat pad that is thicker and better engineered than the tissue under the ball of the foot. A true heel bruise usually follows something you can name: a hard landing, a barefoot step onto gravel, a jump down from a tailgate. It is tender in the middle of the heel pad, it is worst on hard flooring, and it resolves on the timeline set out below.
Three other things imitate it closely. Heel fat pad atrophy produces central heel soreness that is worst barefoot on tile or hardwood and much better in a cushioned shoe, but it arrives gradually with no single incident behind it. Plantar fasciitis sits at the front and inner corner of the heel rather than dead center, is worst on the first few steps out of bed or after sitting a while, and eases off as the foot warms up. Neither one follows the pattern of an impact injury.
The third imitator is a calcaneal stress reaction, an overload injury of the heel bone itself, and there is a useful test for it you can do sitting down. Cup the heel between both palms and squeeze firmly from the sides. A bruised fat pad is largely indifferent to side-to-side pressure, because the sore tissue is underneath rather than between your hands. A stressed heel bone is not indifferent at all. A positive squeeze test is a reason to be seen rather than to keep waiting it out.
Burning or tingling that spreads forward from the inner heel toward the arch is a fourth pattern and not a bruise at all; that combination points at nerve irritation, which responds to footwear chosen for tarsal tunnel syndrome rather than to more cushioning.
Offloading the heel is also not the same job as offloading the forefoot, and the products do not transfer. A metatarsal pad does nothing for a sore heel. What helps is a contoured heel cup or a cushioned heel insert that spreads load off the center of the pad, paired with a shoe that has real material under the rearfoot. If the soreness has been going on long enough that you are reading about it, the broader workup for heel pain is the right next step.
In the arch
The arch is the one location where the description does not fit the anatomy. There is very little fat pad under the arch, because the arch is not built to be a weight-bearing contact point in the first place, so there is not much there to bruise. A deep bruise-like ache through the middle of the sole is therefore usually something else wearing the same disguise.
The likely candidates are a strain along the plantar fascia where the band runs forward from the heel, a plantar fibroma, which is a firm nodule sitting within that band and tends to hurt when the edge of an insole presses into it (see shoes that work around a plantar fibroma), and, less often than people fear but often enough to be worth checking, a genuine foreign body that entered the skin and sealed over behind itself. If you can feel a discrete lump under your fingertip, you are not dealing with a bruise.
Under the ball of the foot
This is the common one, and it is where the five causes above apply directly. The useful question at this location is not what to call it but which metatarsal head it sits under, whether it feels sharply pinpoint or spread across the whole pad, and whether pushing off makes it worse. Those three answers separate the causes cleanly, and each of them calls for a different pad, a different insole, and a different amount of patience.
How Long Does a Stone Bruise Take to Heal?
Healing time depends entirely on the underlying cause:
- True bone contusion (direct impact): 1–3 weeks with rest and cushioning
- Metatarsalgia: 2–6 weeks with proper orthotic intervention and load reduction
- Plantar fat pad atrophy: Symptom management is ongoing — the pad does not regenerate
- Plantar plate tear (partial): 6–12 weeks with taping and offloading; complete tears may require surgery
- Morton’s neuroma: Varies — mild cases improve within weeks of shoe modification; significant neuromas require injection or surgery
- Sesamoid stress fracture: 6–12 weeks of offloading in a removable walking boot
⚠️ Stone bruise red flags requiring prompt evaluation
- Pain persisting or worsening after 4 weeks of relative rest and cushioning
- Point tenderness precisely over a metatarsal shaft (not at the head) — stress fracture until imaged
- Visible swelling, bruising, or an inability to bear weight after a specific impact — acute fracture
- Diabetic or neuropathic patient with any forefoot pain — high ulcer risk, needs professional evaluation
- A palpable nodule or lump under the metatarsal head that does not resolve — plantar fibroma or neuroma
Treatment and Home Care
For initial management of forefoot stone bruise pain before a diagnosis is established:
- Metatarsal pad: A small adhesive or orthotic-mounted pad placed just behind the painful area distributes load away from the sore metatarsal head. This is the single most effective non-prescription intervention for metatarsalgia and stone bruise pain.
- Cushioned insoles: Full-length insoles with a foam or gel forefoot cushion reduce peak plantar pressure. Particularly helpful for fat pad atrophy.
- Rocker-bottom shoes: Footwear with a curved rocker sole (as opposed to flexible sole) reduces the peak load on the metatarsal heads at toe-off by 30–40% in some studies.
- Relative rest: Reduce high-impact activities. Substitute cycling or swimming temporarily.
- Ice: 15–20 minutes after activity to reduce local inflammation.
What to avoid: thin-soled footwear, high heels, walking barefoot on hard floors, and any activity that consistently provokes the pain above a mild level.
MOST COMMON MISTAKE WE SEE
Patients treat recurrent stone bruise pain with metatarsal pads and cushioned shoes, get temporary relief, and assume the problem is solved — only to have it return the moment they go back to their usual shoes or activity level. Stone bruise pain that keeps coming back means the underlying mechanical overload has not been addressed. Generic cushioning redistributes pressure slightly but does not correct the root cause. Custom orthotics with a precise forefoot prescription are almost always needed for lasting resolution of recurring stone bruise symptoms.
Stone Bruise, Rock Bruise, Bone Bruise: What the Names Mean
People bring this complaint in under several names. Stone bruise and rock bruise are the same thing, and both describe a sensation rather than an injury. A bruised metatarsal and a bruised sole are that same complaint again, aimed at a slightly different address. None of them is a diagnosis, which is why two people using identical words can leave with two entirely different treatment plans.
Bone bruise is the one term on that list carrying a specific technical meaning, and it is not what most people intend by it. On imaging, a bone bruise is marrow edema: bleeding and swelling inside the bone itself, in the spongy tissue behind the hard outer shell. It does not appear on plain film and shows up only on MRI, and it sits on the same continuum that ends in a stress fracture.
Most stone bruises are not bone bruises in that sense. The damaged tissue is the fat pad and the lining on the outside of the bone, not the marrow inside it, which is why they behave the way they do: sore under load, quiet once the weight comes off, steadily better week over week. A marrow injury is less polite. It aches while you are sitting still, it can wake you at night, and it does not switch off simply because you stopped walking on it.
That difference is the practical one. Discomfort that behaves like a bruise but never lets go of you between steps, in a foot whose plain films came back clean, is the situation where advanced imaging earns its cost. A normal radiograph rules out a great deal less than most patients assume it does.
Frequently Asked Questions: Stone Bruise on the Foot
What is a stone bruise on the foot?
A stone bruise is a deep contusion to the fat pad beneath the metatarsal heads — the protective cushioning under the ball of the foot. It’s caused by stepping forcefully on a hard, pointed object. The result is localized pain directly under the metatarsal head that worsens with direct pressure and weight-bearing.
How long does a stone bruise take to heal?
Most stone bruises heal within 2–6 weeks with conservative care — rest, cushioned insoles, and avoiding bare feet. If pain persists beyond 6 weeks, a stress fracture should be ruled out with X-ray or MRI, as both conditions feel nearly identical.
How do you treat a stone bruise?
Treatment includes a donut-shaped metatarsal pad to offload pressure, cushioned shoes or insoles, NSAIDs for inflammation, and relative rest. Ice 15–20 minutes several times daily helps the acute phase. Most patients recover fully without surgical intervention.
What are the most common causes of heel pain?
Plantar fasciitis accounts for about 80% of heel pain cases. Other causes include heel spurs, Achilles tendinopathy, stress fractures, bursitis, and nerve entrapment. An accurate diagnosis—often confirmed with ultrasound or X-ray—guides the most effective treatment.
How can I tell if my heel pain needs imaging?
X-rays are ordered when trauma is suspected or pain is severe and sudden. Ultrasound is ideal for soft-tissue causes like plantar fasciitis and Achilles tendinopathy. MRI is reserved for suspected stress fractures or nerve entrapment that X-rays cannot detect.
Related reading: broken big toe · protruding bone on outside of foot · Kager triangle fat pad
The American Podiatric Medical Association recommends cushioned heel inserts and activity modification as first-line conservative treatment for plantar fat pad contusion (stone bruise), which affects the heel’s natural shock-absorbing tissue.
📋 Dr. Tom Biernacki, DPM, FACFAS answers:
Most stone bruises on the ball of the foot heal within 2–6 weeks with conservative care: rest, ice, offloading padding, and cushioned footwear. Deep stone bruises over a metatarsal head can take up to 8–10 weeks if activity isn’t modified. If pain doesn’t improve after 3 weeks of rest, or if there was a significant impact injury, an X-ray is warranted to rule out a metatarsal stress fracture — which looks and feels nearly identical to a stone bruise.
The American Academy of Orthopaedic Surgeons notes that localized forefoot and heel pain from impact trauma — commonly called a stone bruise — typically resolves with rest, cushioned footwear, and metatarsal padding within a few weeks of reducing high-impact activity.
Can a stone bruise cause a stress fracture? Repeated stone bruise-like symptoms from overloaded metatarsal heads can indicate the same mechanical forces that cause metatarsal stress fractures. The two conditions exist on a spectrum — chronic metatarsal overload produces periosteal inflammation (“bone bruise”) first, and if the load continues without correction, progresses to a stress reaction and eventually a frank stress fracture. Any stone bruise that worsens over weeks rather than improving warrants X-ray evaluation.
Why does my stone bruise keep coming back in the same spot? Recurrent stone bruise pain in the same location almost always indicates a persistent mechanical overload issue — too much pressure repeatedly concentrating on one metatarsal head. This is the hallmark of a structural foot problem: a long second metatarsal, first ray hypermobility (bunion-related), metatarsal declination angle abnormality, or fat pad depletion. Custom orthotics specifically designed for your foot’s pressure map are the definitive solution for recurrent forefoot stone bruise pain.
Does ice help a stone bruise? Ice reduces local periosteal inflammation and provides analgesic relief. Use 15–20 minutes 2–3 times daily, with a thin cloth between the ice pack and skin. Ice is most helpful in the first 48–72 hours and as a post-activity recovery measure. It does not accelerate structural healing — that requires load reduction.
Footwear & Orthotics for a Stone Bruise
A stone bruise on the ball of the foot heals faster when you offload it. Cushioned podiatrist-recommended shoes and metatarsal-pad orthotics take pressure off the spot. See a podiatrist if pain lingers beyond a couple of weeks.
Ready to Get Relief?
Same-day appointments available in Howell & Bloomfield Hills, MI
4.9★ | 1,123 Reviews | 3,000+ Surgeries
Or call: (810) 206-1402
For a complete clinical overview: Heel Pain Causes & Treatment Guide — every cause of foot and heel pain diagnosed
Deep, bruise-like pain in your sole that won’t heal?
A “stone bruise” can be a bruised fat pad, a stress fracture, or a nerve problem — each treated very differently. In Michigan? our podiatrists can pinpoint it and get you out of pain. Same-week visits in Howell & Bloomfield Hills, most insurance accepted.
📅 Book an Appointment 📞 (810) 206-1402★ 4.9 from 1,123+ Google reviews · Same-week visits · We verify your insurance free — most visits are just a copay.
Stone Bruise or Something Else? Sorting the Look-Alikes
A true stone bruise is a contusion of the fat pad and underlying bone, and it behaves predictably: it follows a moment you can usually remember, and it improves steadily over two to three weeks once you offload it. When the pain has no clear starting incident, or when it is not clearly better after two weeks, the differential matters. Several common conditions produce nearly identical deep, bruise-like pain under the foot, and each one is managed with a different shoe, insole, and activity plan.
- Aching under the ball of the foot that builds through the day — this is more typical of metatarsalgia than a bruise, because it tracks with cumulative load rather than a single impact. Offloading the metatarsal heads is the fix: see shoes built for metatarsalgia and the insole design that actually redistributes forefoot pressure.
- Pinpoint pain beneath the big toe joint, worst as you push off — the two sesamoid bones sit directly under that joint and bruise or inflame in isolation. That is sesamoiditis, and it needs a stiffer forefoot, not more cushioning.
- Pain that has worsened over weeks and hurts when you press one specific spot on a bone — treat this as a stress fracture until proven otherwise. Footwear that limits bending through the injured segment matters here; see shoe selection during a stress fracture.
- Sharp heel pain on the first few steps in the morning that eases as you walk — that pattern is characteristic of plantar fasciitis rather than a contusion, and it responds to a completely different approach.
- Pain that reliably returns whenever you are back on concrete or tile all day — the tissue is not failing, the surface is. This is a load problem best solved with insoles designed for all-day standing on hard floors.
One caution worth stating plainly: a stress fracture is frequently invisible on an initial X-ray for the first two to three weeks, which is exactly why a persistent “stone bruise” is one of the more commonly missed foot injuries. If you cannot bear weight comfortably, if bruising is spreading, or if the pain is trending worse rather than better after two weeks, that warrants an in-person exam and appropriate imaging rather than another week of waiting. You can reach our Howell and Bloomfield Hills offices at (810) 206-1402.
When a stone bruise needs a podiatrist
Most stone bruises — a deep contusion of the fat pad under the heel or the ball of the foot — settle within two to four weeks with cushioning, reduced impact and a supportive shoe. What should prompt an in-person exam is pain sharply localized to one metatarsal head rather than spread across the pad, pain that worsens rather than eases over the first two weeks, pain at night, or any inability to bear weight. Those patterns point away from a simple contusion and toward metatarsalgia, a stress fracture or a plantar plate injury, each managed very differently. A weight-bearing X-ray and a hands-on exam usually separate them in a single visit, and persistent fat-pad pain often responds well to custom orthotics that offload the painful area.
Balance Foot & Ankle sees patients at two Michigan offices: our Howell podiatry office, serving Livingston County, and our Bloomfield Hills podiatry office, serving Bloomfield Hills, Birmingham, Pontiac and the rest of Oakland County. Dr. Tom Biernacki sees patients at both. Call (810) 206-1402 to book an appointment.
The Bottom Line
A stone bruise that resolves within 2 weeks of rest and cushioning almost certainly was a simple bone contusion. A stone bruise that persists, recurs in the same spot, or gradually worsens is telling you something structural about how your foot is loading — metatarsalgia, fat pad loss, plantar plate injury, or the early stages of a stress fracture. The sooner we identify which, the sooner we can correct the underlying mechanical cause rather than just managing symptoms.
If you’ve been living with the pebble-under-the-foot feeling for more than 3–4 weeks, a single diagnostic visit to our Howell or Bloomfield Hills office will identify the cause and get you started on the correct treatment path.
Sources
- Espinosa N, Brodsky JW, Maceira E. Metatarsalgia. J Am Acad Orthop Surg. 2010;18(8):474-485.
- Espinosa N, Maceira E, Myerson MS. Current concept review: metatarsalgia. Foot Ankle Int. 2008;29(8):871-879.
- Grebing BR, Coughlin MJ. The effect of ankle position on the exam for first ray mobility. Foot Ankle Int. 2004;25(7):467-475.
- Jastifer JR, Gustafson PA. The impact of plantar fascia release on plantar pressure. Foot Ankle Int. 2012;33(12):1098-1101.
- Trnka HJ, Nyska M, Parks BG, Myerson MS. Dorsiflexion contracture after the Weil osteotomy: results in vitro analysis. Foot Ankle Int. 2001;22(1):47-50.
Book an appointment with a podiatrist
Deep bruising in the ball or heel of the foot that has not settled after a couple of weeks is worth an X-ray, because a stress fracture and a stone bruise can feel much the same and are managed very differently. Balance Foot & Ankle sees patients at two offices — Howell in Livingston County, and Bloomfield Hills in Oakland County.
Call (810) 206-1402 or use the form below and our team will find you an appointment time.
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.
More questions patients ask
How do I treat a stone bruise at home?
Rest the foot, apply ice for 15–20 minutes several times daily, wear cushioned shoes, and take NSAIDs like ibuprofen. If pain persists beyond 3 weeks, see a podiatrist to rule out stress fractures or other causes.
How do you treat a stone bruise at home?
Stone bruise home treatment: ice 15 min 3-4x daily for 48 hours, NSAIDs for 5-7 days, supportive shoes with heel cup or gel insert (no barefoot), elevation when seated, gradual return to activity. Avoid: barefoot walking, hard surfaces, running for 2-3 weeks. If pain prevents weight-bearing, see a podiatrist for evaluation.
How do I know if I have a stone bruise or stress fracture?
Stone bruises hurt most with direct pressure at the impact point and improve significantly within a week of rest. Stress fractures hurt with activity even without direct impact, may have pinpoint tenderness along the bone (not just the pad), and often show the tuning fork test positive (vibration worsens pain). A stone bruise that is not improving after 2 weeks, is getting worse, or is accompanied by swelling or bruising warrants imaging to rule out a stress fracture.
Still have a question about coverage or cost? Call (810) 206-1402 and we will check your benefits before you come in — or book online: Book in Howell · Book in Bloomfield Township