
Quick answer: Tendon Transfer Surgery Drop Foot Posterior Tibial is a common foot/ankle topic that affects many patients. The 2026 evidence-based approach combines proper diagnosis, conservative-first treatment, and escalation only when needed. We treat this regularly at our Howell and Bloomfield Township practices. Call (810) 206-1402.
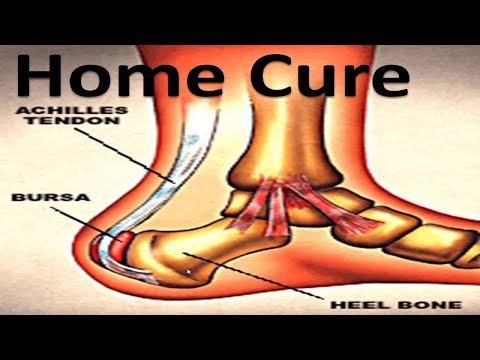
Watch: Heel Bursitis & Achilles Tendon Bursitis [Best HOME Treatment!] — MichiganFootDoctors YouTube
Medically reviewed by Dr. Tom Biernacki, DPM — Board-Certified Podiatric Surgeon — Balance Foot & Ankle, Howell & Bloomfield Hills, MI. Last updated April 2026.
Medically reviewed by Dr. Tom Biernacki, DPM — Board-certified podiatric surgeon at Balance Foot & Ankle Specialists, serving Howell and Bloomfield Hills, Michigan.
Quick Answer: Tendon transfer surgery reroutes a functioning tendon to replace the action of a paralyzed or weakened tendon in drop foot. The posterior tibial tendon is most commonly transferred to restore dorsiflexion. Recovery takes 3 to 6 months with physical therapy, and most patients achieve significant improvement in gait and function.

What Is Tendon Transfer Surgery?
A tendon transfer involves detaching a tendon from its normal insertion point and reattaching it to a new location where it can perform a needed function. The transferred tendon must be expendable (its original function can be compensated by remaining tendons), of adequate strength, and oriented appropriately to produce the required motion at the new attachment site.
Tendon transfers differ from tendon repairs (suturing a torn tendon back together) and tendon grafts (using donor tissue to bridge a gap). In a transfer, the entire musculotendinous unit — the muscle and its tendon — is redirected to a new purpose.
The biological principle is elegant: the transferred muscle-tendon unit gradually re-educates to perform its new function through physical therapy and neuromuscular retraining. Most patients achieve functional reinnervation of the transfer within 3–6 months.
When Is Tendon Transfer Recommended?
Tendon transfer surgery is indicated when:
- A tendon is irreparably ruptured and cannot be primarily repaired (e.g., chronic, retracted Achilles or posterior tibial tendon tears)
- A muscle is paralyzed due to nerve injury (e.g., foot drop from peroneal nerve palsy)
- Tendon imbalance is causing structural deformity (e.g., claw toe, flatfoot, cavus foot)
- A tendon has been destroyed by infection, trauma, or tumor excision
- Primary repair has failed and the patient remains symptomatic
Contraindications include poor skin and soft tissue quality, active infection, severe arterial insufficiency, and patients who are poor surgical candidates for other medical reasons.

Common Foot Tendon Transfer Procedures
Posterior Tibial Tendon Reconstruction (Flatfoot Repair)
The most commonly performed tendon transfer in the foot. When the posterior tibial tendon (PTT) is irreparably torn, the flexor digitorum longus (FDL) tendon is transferred to take over PTT’s arch-supporting function. This is typically combined with bone procedures (calcaneal osteotomy, lateral column lengthening) to fully correct the flatfoot deformity.
Peroneus Longus to Brevis Transfer
When the peroneus brevis tendon (primary ankle evertor) is torn and cannot be repaired, the peroneus longus is transferred to restore eversion strength and ankle stability — particularly important after chronic lateral ankle instability with tendon involvement.
Tendon Transfer for Foot Drop (Tibialis Anterior Insufficiency)
When the anterior tibial muscle/tendon is paralyzed (often from peroneal nerve palsy, drop foot from L4-L5 disc disease, or post-compartment syndrome), the tibialis posterior tendon is transferred through the interosseous membrane to the dorsum of the foot to restore dorsiflexion and eliminate foot drop.
Flexor-to-Extensor Transfer for Claw and Hammer Toes
A flexor tendon (FDL or FDB) from the plantar aspect of the toe is routed to the extensor mechanism on the dorsum. This balances the intrinsic-extrinsic muscle imbalance driving the deformity, straightening the toe without fusion in appropriately selected patients.
Modified Achilles Reconstruction (FHL Transfer)
For large or chronic Achilles tendon defects that cannot be primarily repaired, the flexor hallucis longus (FHL) tendon is transferred into the calcaneus to augment or reconstruct Achilles function. Often combined with a V-Y advancement or turndown flap.
What Happens During Surgery
Tendon transfer surgery is performed under general or regional (nerve block) anesthesia, typically as an outpatient procedure. The surgical steps include:
- Harvesting the donor tendon: The tendon to be transferred is released from its insertion point while preserving its musculotendinous junction and neurovascular supply
- Preparing the recipient site: A bone tunnel or soft tissue channel is created at the new attachment site
- Tensioning: The tendon is passed to its new location and tensioned appropriately — too loose or too tight results in poor function
- Fixation: The tendon is secured using an interference screw, suture anchor, or bone tunnel suture technique
- Concomitant procedures: Bone osteotomies, joint fusions, or ligament repairs are performed as needed to address the structural cause
Recovery and Rehabilitation Timeline
Recovery from tendon transfer surgery is longer than simpler foot procedures because the transferred tendon requires neuromuscular re-education — the brain must learn to activate the muscle for its new purpose.
Weeks 0–6: Non-weight-bearing phase. The foot is immobilized in a splint or cast to protect the tendon fixation during initial healing. Crutches or a knee scooter are required. Swelling management is critical.
Weeks 6–12: Transition to weight-bearing. A CAM boot allows gradual return to weight-bearing. Physical therapy begins with range of motion, edema control, and gentle muscle activation exercises for the transferred tendon.
Months 3–6: Strengthening and re-education. Intensive physical therapy focuses on retraining the transferred muscle for its new function, progressive strengthening, and functional movement patterns. Most patients return to normal shoe wear and daily activity by month 4–5.
Months 6–12: Return to full activity. Return to sports and high-demand activities is individualized. Final functional outcomes are typically assessed at 12 months.
Recovery Support Products
These products help manage pain, swelling, and functional recovery during the months following tendon transfer surgery.
Disclosure: This page contains affiliate links. We may earn a small commission at no cost to you. We only recommend products Dr. Biernacki trusts for his own patients.
Transition Insoles: PowerStep Pinnacle
As you transition out of the surgical boot and back into regular footwear, PowerStep Pinnacle Orthotic Insoles provide the arch support and cushioning your foot needs while the transferred tendon is still remodeling and gaining strength.
The structured arch support reduces compensatory strain on the healing tendon transfer and adjacent structures. The dual-layer EVA base cushions impact during the early return-to-walking phase. Dr. Biernacki routinely recommends PowerStep Pinnacle as a transition insole after flatfoot reconstruction with FDL transfer and after peroneal tendon procedures.
Pain and Swelling Relief: Doctor Hoy’s Natural Pain Relief Gel
Post-surgical aching and stiffness are expected during tendon transfer recovery. Doctor Hoy’s Natural Pain Relief Gel provides targeted topical relief over the surgical site and surrounding musculature without systemic NSAID effects — important during the healing phase when tissue integrity is critical.
Apply Doctor Hoy’s to the incision perimeter (not over open wounds) and adjacent tendons during the transition and strengthening phases. It’s particularly helpful for managing Achilles and calf soreness during the neuromuscular re-education phase of physical therapy.
Edema Control: DASS Compression Socks
Post-surgical edema is one of the most limiting factors in tendon transfer recovery — swelling stiffens the surgical site, impairs range of motion, and slows physical therapy progress. DASS Compression Socks at 15–20 mmHg graduated compression are recommended once the surgeon approves compression use (typically after wound healing, around weeks 4–6).
DASS compression helps control dependent edema during the transition to weight-bearing, supports the venous return that is critical for tissue healing, and provides mild proprioceptive feedback during early ambulation exercises.
🧰 The Complete Tendon Transfer Recovery Kit
Dr. Biernacki’s recommended three-product protocol for the transition and strengthening phases of tendon transfer recovery:
- PowerStep Pinnacle — transition arch support as you return to regular footwear after the surgical boot
- Doctor Hoy’s Natural Pain Relief Gel — topical pain and stiffness relief during rehabilitation
- DASS Compression Socks — post-surgical edema control once wound is healed (surgeon approval required)
🚨 Warning Signs During Tendon Transfer Recovery
Contact Dr. Biernacki’s office immediately or go to urgent care if you experience:
- Sudden loss of the correction — the deformity returning or foot drop reappearing may indicate tendon re-rupture or fixation failure
- Wound dehiscence (opening of the surgical incision) or drainage
- Signs of deep infection: increasing pain, warmth, swelling, fever, red streaking from the wound
- Calf pain with swelling and warmth — possible DVT (deep vein thrombosis), which requires immediate evaluation
- Sudden sharp pain with a pop during physical therapy — possible re-rupture of the transfer
- Pressure sores or skin breakdown under the cast or boot
🔑 The Most Common Recovery Mistake
Returning to activity too early because the foot “feels fine.” Tendon transfers feel surprisingly comfortable in the early weeks — especially once the post-op swelling subsides. But the mechanical strength of the tendon fixation lags well behind subjective comfort. The bone tunnel or suture anchor requires 8–12 weeks to achieve full biological integration. Patients who advance activity too quickly risk partial fixation failure, re-rupture, and loss of the correction. Follow your surgeon’s protocol exactly, even if you feel ready earlier.
Watch: Foot Tendon Transfer Surgery Explained

Treatment Bridge: Related Conditions and Procedures
- Adult Flatfoot Reconstruction — FDL tendon transfer is a core component
- Posterior Tibial Tendon Dysfunction — the most common indication for tendon transfer
- Achilles Tendon Rupture — FHL transfer for chronic or large defects
- Hammer Toe and Claw Toe Surgery — flexor-to-extensor transfer for flexible deformities
Important: Tendon transfer surgery requires a dedicated rehabilitation period of 3 to 6 months. Patients must commit to physical therapy and gradual return to weight-bearing. Success depends significantly on the underlying cause of drop foot, the duration of nerve damage, and compliance with the post-operative protocol.
Frequently Asked Questions About Tendon Transfer Surgery
How long does tendon transfer surgery take?
Tendon transfer surgery typically takes 1–2 hours depending on the specific procedure and whether concomitant bone work is required. Most foot tendon transfers are performed as outpatient procedures under general or regional anesthesia with same-day discharge.
How painful is tendon transfer recovery?
Pain is well-controlled with a nerve block (which provides 12–24 hours of excellent analgesia) and oral pain medications. The first 72 hours are the most uncomfortable. After that, most patients report manageable discomfort managed with over-the-counter analgesics. The prolonged recovery is less about pain and more about activity restriction and rehabilitation.
Will the transferred tendon work normally?
Transferred tendons work well but rarely perfectly. Most patients achieve excellent functional improvement — the primary goal is restoring balanced, pain-free walking mechanics, not recreating the precise biomechanics of the original tendon. Physical therapy is essential for re-educating the transferred muscle for its new role, and most patients are very satisfied with functional outcomes.
What are the risks of tendon transfer surgery?
Risks include infection, nerve or vessel injury, wound healing complications, DVT, and tendon re-rupture or fixation failure. Loss of donor tendon function (weakness in the original action of the transferred tendon) is expected and should be discussed with your surgeon. Overall complication rates are low when surgery is performed by an experienced foot and ankle specialist.
Do I need physical therapy after tendon transfer?
Yes — physical therapy is not optional after tendon transfer surgery. It is essential to regain range of motion, control post-surgical edema, and most importantly to re-educate the transferred tendon for its new function. Patients who skip or minimize physical therapy have significantly worse functional outcomes.
Differential Diagnosis: What Else Could It Be?
Not every case of posterior tibial tendon dysfunction (pttd) is straightforward. In our clinic we routinely rule out three look-alike conditions before confirming the diagnosis. If your symptoms don’t match the classic presentation, one of these may explain the pain — which is why physical exam matters more than self-diagnosis.
| Condition | How It Differs |
|---|---|
| Congenital flat foot | Lifelong, usually bilateral, no pain, normal single-leg heel-rise test. |
| Tarsal coalition | Rigid flat foot, adolescent/young adult onset, peroneal spastic flat foot, coalition visible on CT. |
| Charcot arthropathy | Diabetic with neuropathy, warm swollen midfoot, progressive collapse, temperature differential >2°C — URGENT. |
Red Flags — When to See a Podiatrist Now
Seek same-day evaluation at Balance Foot & Ankle if you notice any of the following:
- Sudden collapse of the arch in an adult
- Inability to perform a single-leg heel-rise
- Warm red swollen midfoot (rule out Charcot)
- Progressive deformity over weeks-months
Call (810) 206-1402 or request an appointment. Our Howell and Bloomfield Hills offices reserve same-day slots for urgent foot and ankle issues.
In Our Clinic: What We See
Clinical perspective from Dr. Tom Biernacki, DPM — Balance Foot & Ankle, Howell & Bloomfield Hills, MI:
In our clinic, adult acquired flatfoot from PTTD typically presents in women over 40, often with recent weight gain or a period of increased standing. They describe medial ankle pain and progressive “collapse” of the arch on one side. The gold-standard exam finding is an inability to perform a single-leg heel-rise on the affected side — the tendon can no longer invert the heel into a rigid lever. Early PTTD is staged and treated with custom orthoses and bracing, but progressive disease (Stage III-IV) typically requires surgical reconstruction to prevent rigid deformity.
Sources
- Myerson MS. “Adult Acquired Flatfoot Deformity: Treatment of Dysfunction of the Posterior Tibial Tendon.” Journal of Bone & Joint Surgery. 1996;78(5):780-792.
- Haddad SL, et al. “Posterior Tibial Tendon Dysfunction: An Exploration of Potential Etiologies.” Foot & Ankle International. 2003;24(1):2-10.
- Raikin SM, et al. “Reconstruction of the Achilles Tendon.” Journal of the American Academy of Orthopaedic Surgeons. 2017;25(9):635-646.
- Bibbo C, et al. “Peroneal Tendon Tears.” Foot & Ankle Clinics. 2000;5(4):833-845.
- Deland JT. “Adult-Acquired Flatfoot Deformity.” Journal of the American Academy of Orthopaedic Surgeons. 2008;16(7):399-406.
Dealing With Drop Foot?
Dr. Tom Biernacki performs tendon transfer surgery for drop foot at Balance Foot & Ankle Specialists in Howell and Bloomfield Hills, Michigan.
Book Your ConsultationCall (810) 206-1402 | Same-day appointments available
Drop Foot Surgery in Michigan
Posterior tibial tendon transfer can restore the ability to lift the foot in patients with permanent foot drop. Our podiatric surgeons perform tendon transfer procedures at our Howell and Bloomfield Hills offices.
Learn About Tendon Surgery | Book Your Appointment | Call (810) 206-1402
Clinical References
- Hove LM, Nilsen PT. Posterior tibial tendon transfer for drop foot. Foot Ankle Int. 2000;21(8):612-614.
- Wagenaar FC, Louwerens JW. Posterior tibial tendon transfer: results of fixation to the dorsiflexors proximal to the ankle joint. Foot Ankle Int. 2007;28(11):1128-1142.
- Shah RK. Tibialis posterior transfer by interosseous route for the correction of foot drop. Int Orthop. 2009;33(4):1137-1141.
Insurance Accepted
BCBS · Medicare · Aetna · Cigna · United Healthcare · HAP · Priority Health · Humana · View All →
Howell Office
3980 E Grand River Ave, Suite 140
Howell, MI 48843
Get Directions →
Bloomfield Hills Office
43700 Woodward Ave, Suite 207
Bloomfield Hills, MI 48302
Get Directions →
Your Board-Certified Podiatrists



Ready to Get Back on Your Feet?
Same-week appointments available at both locations.
Book Your AppointmentWatch: Tendon Transfer Surgery for Drop Foot
Dr. Tom on drop-foot tendon transfer — posterior tibial transfer through interosseous membrane, Bridle procedure, AFO retirement, recovery (6-12 months), outcomes.

Post-Transfer Recovery Kit
Structured gait re-education. Dr. Tom’s kit:
As an Amazon Associate, Balance Foot & Ankle earns from qualifying purchases. This supports our free patient education content.
Weeks 1-12 protection.
Weeks 12-26 return-to-shoe.
Tendon healing support.
Topical front-ankle relief.
Related: Drop Foot Surgery · Surgery Services · Book Drop Foot Consultation
In-Office Treatment at Balance Foot & Ankle
When conservative care isn’t enough, Dr. Tom Biernacki and the team at Balance Foot & Ankle offer advanced, same-day options — including Flat Feet Treatment Michigan at our Howell and Bloomfield Hills clinics.
Same-day appointments available. Call (810) 206-1402 or book online.
Frequently Asked Questions
When should I see a podiatrist?
If symptoms persist past 2 weeks, affect your normal activity, or are accompanied by red-flag symptoms (warmth, redness, swelling, inability to bear weight).
What does treatment cost?
Most diagnostic visits and conservative treatments are covered by Medicare and major insurers. Out-of-pocket costs vary by your specific plan.
How quickly can I get an appointment?
Most non-urgent cases see us within 5 business days. Urgent cases (sudden pain, possible fracture) typically same or next business day.
Dr. Tom Biernacki, DPM is a double board-certified podiatrist and foot & ankle surgeon at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has reached over one million views.
- Diagnosis and Treatment of Plantar Fasciitis (PubMed / AAFP)
- Heel Pain (APMA)
- Hallux Valgus (Bunions): Evaluation and Management (PubMed)
- Bunions (Mayo Clinic)