

The most important clinical decision with Peroneal Tendonitis Treatment isn’t which treatment to start with &#
No products found.
8212; it’s identifying the correct subtype. That changes everything. Call (810) 206-1402.Peroneal Tendon Disorders: Tendinitis vs. Tendinopathy vs. Tear — What’s the Difference?
The terms “peroneal tendonitis” and “peroneal tendinopathy” are often used interchangeably — but they represent different stages of the same condition, with different treatment implications. And both are distinct from a peroneal tendon tear, which may require surgery. Getting the right diagnosis determines whether you need rest and rehab, or imaging and surgical consultation.
| Condition | Pathology | Clinical Presentation | Imaging | Treatment |
|---|---|---|---|---|
| Peroneal tendinitis (acute) | Acute inflammatory response in the peroneus longus or brevis tendon; often following a single overuse event or ankle sprain; early-stage with intact tendon architecture | Lateral ankle and posterior fibula pain; tenderness along the tendon course behind the fibula and below the lateral malleolus; swelling along the tendon sheath; pain with resisted foot eversion; onset correlates with recent activity increase or ankle injury | Ultrasound: tendon sheath effusion (fluid around tendon), mild tendon thickening; MRI: peritendinous edema; tendon structurally intact | Rest (relative — reduce aggravating activity); ice; NSAIDs (short course); functional ankle brace; physical therapy — eccentric loading, peroneal strengthening, proprioception; orthotics for lateral arch support; most acute cases resolve in 4-8 weeks |
| Peroneal tendinopathy (chronic) | Degenerative changes in the tendon substance (not primarily inflammatory); collagen fiber disorganization; intratendinous neovascularization; no acute inflammatory cells on histology; results from repetitive microtrauma without adequate recovery | Chronic lateral ankle pain >6 weeks; pain with activity that partially resolves at rest; tendon may feel thickened or nodular on palpation; morning stiffness; no resolution despite standard rest; snapping sometimes present if subluxation component | Ultrasound: tendon thickening, loss of fibrillar echotexture, intratendinous hypoechoic areas (neovascularization on Doppler); MRI: intratendinous signal change; longitudinal splits possible | Eccentric loading protocol (12-week program); shockwave therapy; PRP injection for resistant cases; aggressive PT; surgery considered for cases >6 months refractory to conservative treatment |
| Peroneus brevis longitudinal split tear | Longitudinal (horizontal) split in the peroneus brevis tendon substance — the most common peroneal tendon tear; often occurs at the fibular groove where the tendon is compressed; frequently associated with ankle instability (chronic lateral ankle sprain) | Chronic lateral ankle pain; snapping behind the lateral malleolus with ankle motion (HIGHLY specific for this diagnosis); pain directly over the peroneus brevis behind the fibula; often history of recurrent ankle sprains; tenderness at the fibular groove | MRI: C-shaped or boomerang morphology of the peroneus brevis (normal = oval); split visible as intratendinous cleft; peroneus longus may bowstring through the split. Ultrasound: dynamic exam shows the split with ankle motion | Small, stable tears: conservative (brace, PT, activity modification); 50-60% respond to conservative treatment. Larger or symptomatic tears: surgical debridement + primary repair (tubularization); groove deepening if fibular groove is too shallow; superior peroneal retinaculum repair if subluxation present; 85-90% good outcomes |
| Peroneus longus tear / os peroneum fracture | Less common; tear at the cuboid tunnel (most vulnerable point for PL); often associated with os peroneum (accessory ossicle in the PL tendon) that can fracture; cuboid avulsion fracture possible | Lateral plantar foot pain (not just ankle — differentiates from PB tear); pain at the cuboid level; pain with forced plantarflexion + inversion; snapping at the cuboid tunnel; os peroneum tenderness | X-ray: os peroneum present ± fracture or displacement (compare bilateral); MRI: PL tear at cuboid tunnel; discontinuity in tendon substance | Os peroneum fracture: immobilization first; surgical excision if painful fragment; PL complete tear: surgical repair or reconstruction depending on tear extent and functional demands |
Peroneal Tendonitis Treatment Protocol: 8-Week Conservative Rehabilitation
| Phase | Timeline | Goal | Exercises / Interventions | Activity Level |
|---|---|---|---|---|
| Phase 1 — Load reduction | Weeks 1-2 | Reduce acute pain and inflammation; protect tendon from further loading | Relative rest from aggravating activities; functional ankle brace (lace-up or stirrup); ice 15 min 3× daily; ankle ROM exercises (pain-free range only); ankle pumps to reduce swelling; NSAIDs if acute (5-7 days maximum) | Walking in functional brace; no running, jumping, lateral cutting; sports that require ankle eversion force eliminated temporarily |
| Phase 2 — Range of motion + isometric strengthening | Weeks 2-4 | Restore full ankle ROM; begin loading the peroneal tendons isometrically | Ankle circles; single-leg balance training (eyes open, then closed); isometric eversion against wall (no movement, just gentle sustained contraction); towel scrunches for intrinsic strength; gentle calf stretching (gastrocnemius + soleus) | Walking tolerated; stairs with handrail; stationary cycling if pain-free |
| Phase 3 — Eccentric peroneal loading | Weeks 4-6 | Rebuild peroneal tendon strength and tissue quality; eccentric loading is the most evidence-supported treatment for tendinopathy | Theraband eversion (concentric + eccentric); single-leg heel raise with eversion emphasis; lateral band walks; BOSU balance; resisted eversion with weight or band; ice after loading sessions | Walk + light jog if pain ≤3/10; no lateral cutting or court sports yet; begin swimming and cycling normally |
| Phase 4 — Functional + sport-specific | Weeks 6-8+ | Full functional recovery; return to sport; prevent recurrence | Lateral agility ladder; single-leg squat; plyometric progressions; sport-specific cutting; custom orthotic with lateral arch support (reduces PL demand); confirm adequate single-leg eversion strength vs. contralateral side | Return to sport with lace-up brace for 3-6 months; return to full activity when pain-free with cutting and plyometrics; brace mandatory for higher-risk activities during return |
Peroneal tendonitis on the outside of the ankle responds to bracing, eccentric exercises, and a slight medial wedge — but the wrong combination can let the tendon worsen instead of heal.
You’re in the right place. Dr. Tom Biernacki, DPM, FACFAS — board-certified foot & ankle surgeon with 3,000+ surgeries — explains exactly what peroneal tendonitis treatment means and what works. Call (810) 206-1402 for same-day appointment at Howell or Bloomfield Hills.
Quick answer: Treatment for peroneal tendonitis treatment follows a stepwise approach: 1) conservative care first (rest, ice, supportive footwear, OTC anti-inflammatories), 2) physical therapy and targeted exercises, 3) in-office treatments (injections, custom orthotics) if conservative fails at 4-6 weeks, 4) surgery for refractory cases. Most patients resolve at step 1 or 2. Call (810) 206-1402.

Medically reviewed by Dr. Tom Biernacki, DPM
Board-certified podiatric surgeon | Balance Foot & Ankle
Last reviewed: May 2026
⭐ #1 Brace for Peroneal Tendonitis
Peroneal tendonitis develops when the tendons running along the outside of the ankle are overstressed — usually by repetitive inversion or supination. The Active Ankle T2 limits lateral ankle movement without restricting forward motion, directly reducing the mechanical load on the inflamed peroneal tendons during every step.
PowerStep Pinnacle Arch Support Insole
⭐ Corrects the Root Cause of Peroneal Tendonitis
In our clinic, overpronation is the #1 mechanical cause of peroneal tendonitis. As the arch collapses inward, the peroneals contract forcefully to compensate — eventually leading to tendon damage. PowerStep insoles control subtalar joint motion, relieving the eccentric load that drives this condition.
Frequently Asked Questions
When should I see a podiatrist?
See a podiatrist if: foot or ankle pain has lasted more than 2–4 weeks without improvement, you’re changing your gait to avoid pain, you have an open wound or sore that isn’t healing, you notice nail discoloration or thickening, you have diabetes and any foot concern, or pain is severe enough to wake you at night. Most foot conditions are easier and cheaper to treat early — what starts as a minor issue can become a surgical problem with months of delay.
What is the difference between a podiatrist and an orthopedic surgeon?
Podiatrists (DPM — Doctor of Podiatric Medicine) specialize exclusively in the foot, ankle, and lower leg. Orthopedic surgeons (MD/DO) have broader musculoskeletal training but variable foot/ankle subspecialization. For foot and ankle-specific problems, a podiatrist often has more focused training and experience. For injuries involving the leg above the ankle, complex pediatric cases, or multi-level reconstruction, orthopedic consultation may be appropriate. We frequently co-manage patients with orthopedic colleagues.
How do I know if my foot pain is serious?
Signs that warrant same-day or next-day evaluation: severe pain that appeared suddenly without clear cause, swelling, redness, and warmth that appeared suddenly (possible gout, infection, or Charcot fracture), an open wound that looks infected (redness spreading, pus, warmth), inability to bear weight, or any foot problem in a diabetic patient. Pain that’s been present for weeks and is stable is important but not an emergency — schedule within 1–2 weeks.
Can foot problems cause back and knee pain?
Yes — this is a kinetic chain effect. Abnormal foot mechanics (overpronation, supination, leg length discrepancy) cause compensatory changes in knee, hip, and lumbar alignment. Roughly 30% of patients presenting to our clinic with knee pain have a treatable foot-level biomechanical cause. Correcting foot mechanics with orthotics or appropriate footwear often provides significant knee and back relief. If you have chronic knee or back pain and haven’t had your foot mechanics evaluated, it’s worth a consult.
Are orthotics worth it?
For the right conditions, yes — custom orthotics are among the most cost-effective interventions in podiatry. They’re most effective for: plantar fasciitis, flat feet with secondary knee/back pain, leg length discrepancy, metatarsalgia, posterior tibial tendon dysfunction, and diabetic foot pressure management. Quality OTC orthotics ($35–60) resolve symptoms for 60% of patients with mild-to-moderate conditions. Custom orthotics are appropriate when OTC options have failed or when the biomechanical problem is complex. We cast custom orthotics in-office.
How do I choose the right running shoes?
Start with your foot type (flat, neutral, high arch) and running pattern (overpronator, neutral, supinator). Flat feet and overpronators do best in stability or motion-control shoes. Neutral feet do well in neutral-cushioned shoes. High arches need maximum cushioning with flexible soles. Always buy running shoes at the end of the day (foot swelling peaks then), get properly fitted by a specialist, and replace every 300–500 miles. If you’ve been injured repeatedly, a gait analysis can identify the mechanical flaw driving your injury pattern.
What is the difference between a sprain and a fracture?
A sprain is a ligament injury (the tissue connecting bones); a fracture is a break in the bone itself. Both can occur with the same trauma (ankle roll, fall). The old test — ‘if you can walk, it’s not broken’ — is wrong; many fractures are initially weight-bearable. Key differences: a fracture typically produces localized bone tenderness along the bone itself, while a sprain is tender over the ligament. X-ray is the standard to differentiate. High-grade sprains without proper treatment can be as disabling as fractures.
How do I prevent foot and ankle injuries?
The four most impactful prevention strategies: (1) Supportive, appropriately fitted footwear for your foot type and activity. (2) Gradual activity progression — the 10% rule (never increase weekly mileage or intensity by more than 10%). (3) Regular calf and ankle mobility work. (4) Strengthening the posterior tibial tendon, peroneals, and intrinsic foot muscles. Most overuse injuries are preventable; most acute injuries are not — but ankle sprain recurrence (60–70% without rehab) is prevented by balance and proprioception training.
Related Conditions
In This Article
- What Is Peroneal Tendonitis?
- Peroneal Tendonitis Treatment: The Step-by-Step Protocol
- When Peroneal Tendonitis Needs Medical Treatment
- Warning Signs That Need Urgent Evaluation
- Frequently Asked Questions
- The Bottom Line
- What is Tendonitis?
- Symptoms and warning signs
- Conservative treatment options
- When is surgery considered?
- Recovery timeline and prevention
What Is Peroneal Tendonitis?
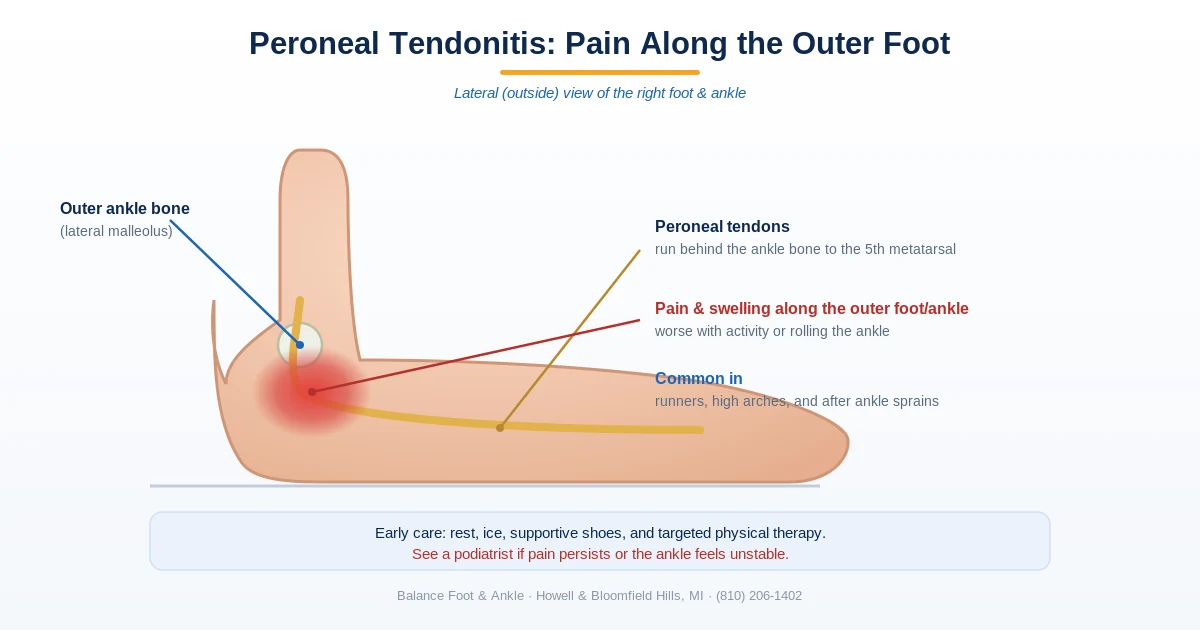
The peroneal tendons run along the outside of your ankle — the peroneus longus and peroneus brevis. Their job is to evert the foot (roll it outward) and stabilize the ankle during walking, running, and lateral movements. Peroneal tendonitis is inflammation and micro-tearing of these tendons, most commonly at the point where they curve behind the lateral malleolus (the outer ankle bone). In our podiatry clinic, we see peroneal tendonitis most often in runners, basketball and tennis players, and people who’ve recently sprained their ankle. The lateral ankle pain it causes is often mistaken for a lingering ankle sprain — but the treatment is different, and getting it right matters for full recovery.
Peroneal Tendonitis Treatment: The Step-by-Step Protocol
Treatment for peroneal tendonitis follows a predictable progression when managed correctly. The key principle: tendons need controlled loading to heal — complete rest actually delays recovery by preventing collagen remodeling. Here’s the protocol we use in our clinic:
- Phase 1 — Acute (Week 1–2): Relative rest from aggravating activities (no running, cutting, or jumping). Ice 15–20 min 3× daily. NSAIDs if tolerated. Lateral ankle bracing (lace-up or semi-rigid) to reduce peroneal tension. Avoid stretching in this phase.
- Phase 2 — Subacute (Week 2–4): Begin isometric and concentric peroneal strengthening with resistance band — ankle eversion exercises. Cross-training with cycling or swimming. Start lateral wedge orthotic to offload the peroneal insertion.
- Phase 3 — Loading (Week 4–6): Progress to eccentric eversion exercises (the most important phase for tendon remodeling). Single-leg balance work. Begin walking at full intensity if pain-free.
- Phase 4 — Return to Sport (Week 6–8+): Sport-specific agility, cutting, and jumping when eccentric strength is at least 90% of unaffected side. Continue bracing for high-demand activity for 2–3 months after return.
Key takeaway: The most common treatment mistake is complete rest followed by sudden return to activity. Tendons heal through progressive loading — the eccentric strengthening protocol is the evidence-backed core of peroneal tendonitis recovery.
When Peroneal Tendonitis Needs Medical Treatment
Most peroneal tendonitis resolves with conservative care. However, some cases require diagnostic imaging and more aggressive treatment. MRI is the gold standard for evaluating the extent of tendon damage — it can distinguish simple tendonitis from a partial or complete peroneal tendon tear, which changes the treatment approach significantly. Ultrasound-guided cortisone injection can provide relief in chronic cases, though it’s used cautiously near tendons due to rupture risk. Platelet-rich plasma (PRP) injection is an emerging option with promising evidence for chronic peroneal tendonopathy.
Warning Signs That Need Urgent Evaluation
⚠️ See a podiatrist promptly if you have:
- A sudden “snap” or pop on the outer ankle followed by significant swelling (possible tendon rupture)
- A visible bump or lump along the peroneal tendon (tendon subluxation or tear)
- Lateral ankle pain that hasn’t improved after 6 weeks of conservative care
- Ankle that gives way repeatedly with lateral movement (instability)
- Recurrent peroneal tendonitis after multiple episodes (suggests underlying structural issue)
The Bottom Line
Peroneal tendonitis is a highly treatable condition when managed with the right protocol. Relative rest, bracing, and progressive eccentric strengthening resolve most cases in 6–8 weeks. The critical mistake is rushing return to sport before the tendon has adequate tensile strength — this is how acute tendonitis becomes a chronic problem. If you’ve had lateral ankle pain for more than 6 weeks, or if you’ve had multiple episodes of what feels like ankle sprains, a podiatric evaluation including ultrasound or MRI can identify whether you’re dealing with tendonitis, a partial tear, or ankle instability — all of which respond differently to treatment.
Sources: Raikin SM et al. (2024). Peroneal tendon disorders. J Am Acad Orthop Surg. | Van Dijk CN et al. (2023). Conservative management of peroneal tendinopathy. Br J Sports Med.
Dr. Tom’s Picks: Peroneal Tendon Recovery
Apply along the lateral ankle and peroneal groove 3-4x daily. Arnica + menthol reduces tendon inflammation topically. Use during active flares.
View on Amazon →
Graduated 20-30mmHg compression reduces lateral ankle swelling and supports the peroneal tendon sheath. Truly graduated — most ankle braces don’t provide this.
View on Amazon →
Peroneal tendonitis from supination needs arch support to stop the lateral heel strike. Pinnacle repositions the foot and reduces lateral column stress.
View on Amazon →
As an Amazon Associate I earn from qualifying purchases. As a Foundation Wellness partner I may also earn commission.
Get Your Peroneal Tendonitis Evaluated
Same-day appointments available in Howell & Bloomfield Hills, MI
4.9★ | 1,123 Reviews | 3,000+ Surgeries
Or call: (810) 206-1402
🦶 Peroneal Tendonitis Recovery Support
- PowerStep Pinnacle Insoles — Peroneal tendonitis is driven by supination (high arches rolling outward) stressing the tendons along the lateral ankle. PowerStep corrects the arch mechanics that drive this loading pattern. Medical-grade OTC.
- Doctor Hoy’s Natural Pain Relief Gel — Apply arnica + camphor directly along the peroneal tendons (outer ankle and below lateral malleolus) 3–4× daily. Reduces tendon sheath inflammation.
Peroneal tendonitis that doesn’t respond in 6–8 weeks may have a partial tear. MRI is the diagnostic gold standard. See ankle & tendon treatment options → · Book → · (810) 206-1402
Watch: Peroneal Tendonitis Treatment — What Actually Works

![Peroneal Tendonitis Treatment 2024 [Peroneus Brevis & Longus Pain!]](https://www.michiganfootdoctors.com/wp-content/cache/flying-press/63da3fd3de394bd1f208c4ae18220dcd.jpg)
Dr. Tom covers the full peroneal tendonitis treatment protocol — from acute phase bracing and activity modification, through targeted strengthening, to when to consider PRP or surgical reconstruction for peroneal tears. The clinical decision points that separate a 6-week recovery from a 6-month one are clearly explained.
Frequently Asked Questions
OrthoInfo – AAOS: Peroneal Tendon Injuries
In-Office Treatment at Balance Foot & Ankle
If you’re dealing with peroneal tendonitis pain on the outer ankle and home care isn’t providing lasting relief, our team at Balance Foot & Ankle provides hands-on exam plus imaging when needed and treatment at our Howell and Bloomfield Hills locations. We use advanced diagnostic tools to determine the exact cause and build a treatment plan tailored to your activity level and goals.
Same-day appointments available. (810) 206-1402
Get Expert Care at Balance Foot & Ankle
Same-week appointments at our Howell and Bloomfield Hills offices. Board-certified podiatric surgeons. Most insurance accepted.
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.