

Quick answer: Treatment for plantar fibromatosis ledderhose disease treatment 2 follows a stepwise approach: 1) conservative care first (rest, ice, supportive footwear, OTC anti-inflammatories), 2) physical therapy and targeted exercises, 3) in-office treatments (injections, custom orthotics) if conservative fails at 4-6 weeks, 4) surgery for refractory cases. Most patients resolve at step 1 or 2. Call (810) 206-1402.
Medically reviewed by Dr. Tom Biernacki, DPM — Board-Certified Podiatric Surgeon — Balance Foot & Ankle, Howell & Bloomfield Hills, MI. Last updated April 2026.
▶ Watch

Medically reviewed by Dr. Tom Biernacki, DPM | Board-certified podiatrist | 3,000+ surgeries performed
Last updated: April 2, 2026
The most important clinical decision with Plantar Fibromatosis Ledderhose Disease Treatment 2 isn’t which treatment to start with — it’s which subtype or underlying cause you actually have. That distinction changes everything. Call us: (810) 206-1402
What Is Plantar Fibromatosis and Why Does It Develop?
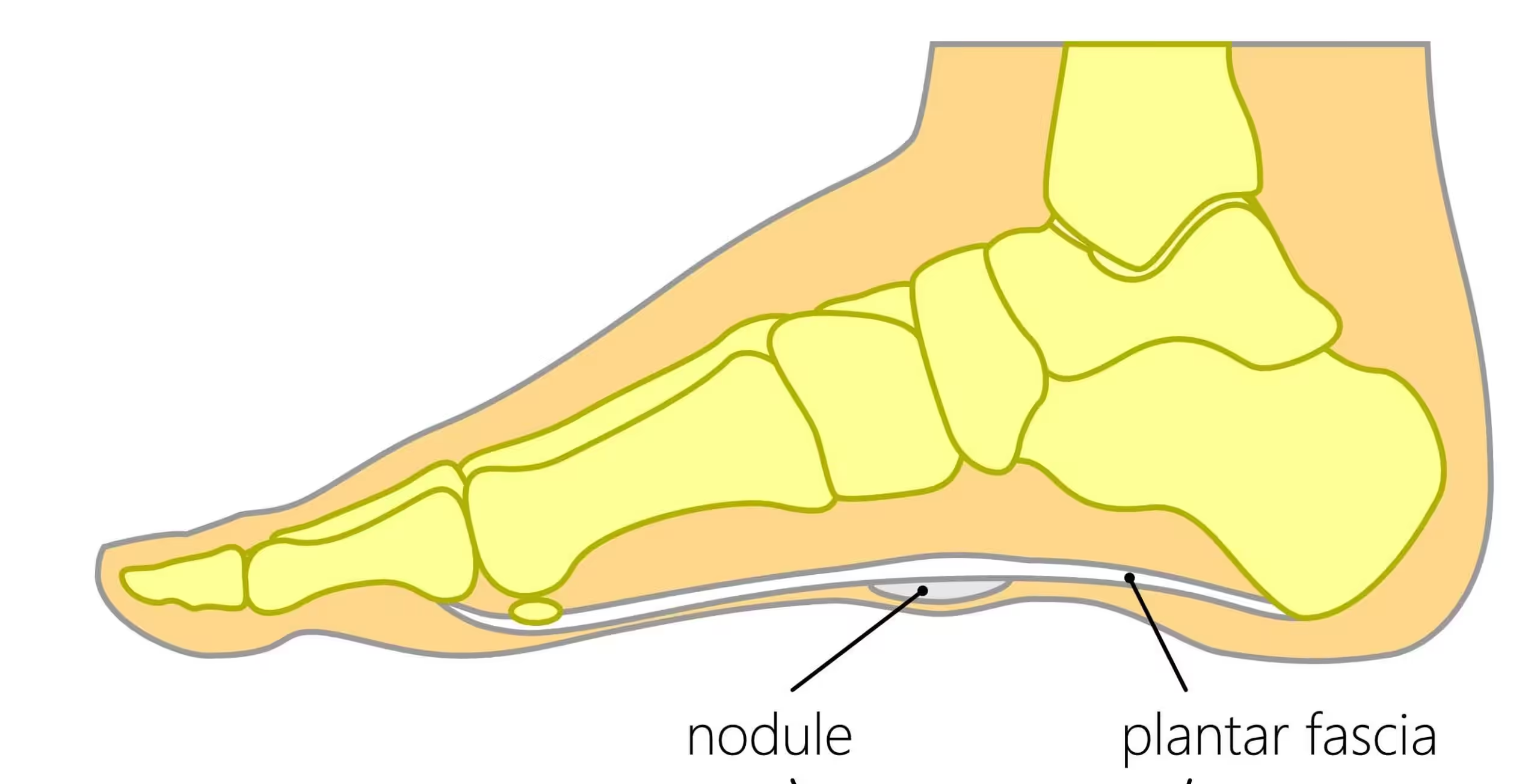
Plantar fibromatosis is a benign fibroproliferative disorder where myofibroblasts infiltrate the central band of the plantar fascia, creating discrete nodules that can grow from pea-sized to several centimeters in diameter. Also known as Ledderhose disease (named after German surgeon Georg Ledderhose who described it in 1894), this condition shares pathological similarities with Dupuytren contracture of the hand and Peyronie disease — all involving abnormal fibroblast proliferation in fascial structures.
The exact cause remains unclear, but genetic predisposition plays a dominant role. Studies show that 60-70% of patients with plantar fibromatosis have a first-degree relative with Dupuytren or related fibromatosis. Northern European ancestry carries the highest risk, with prevalence estimated at 5-25% in populations over age 50. Additional risk factors include chronic liver disease (particularly alcoholic cirrhosis), diabetes mellitus, epilepsy medications (especially phenobarbital), and repetitive plantar trauma.
Nodules typically develop in the medial band of the plantar fascia between the heel and the midfoot. They progress through three phases: the proliferative phase (active fibroblast growth), the active phase (nodule enlargement and possible pain), and the residual phase (mature, stable nodules). Understanding which phase a patient is in guides treatment selection — aggressive therapy during the proliferative phase can prevent progression, while residual-phase nodules may require surgical excision if symptomatic.
Recognizing Plantar Fibromatosis: Signs and Symptoms
The hallmark symptom is a firm, fixed nodule on the bottom of the foot that patients often first notice as a “marble” or “lump” in the arch area. Unlike plantar fasciitis (which causes heel pain primarily in the morning), plantar fibromatosis pain is localized directly over the nodule and worsens with direct pressure — such as standing on hard surfaces, walking barefoot, or wearing thin-soled shoes.
Some patients develop multiple nodules along the plantar fascia, a condition called plantar fibromatosis with cord formation. When nodules enlarge and merge, they can create a fibrous cord that gradually contracts the toes into flexion (similar to Dupuytren contracture in the hand). This toe contracture develops slowly over years but becomes increasingly difficult to reverse without surgical intervention once established.
Differential diagnosis is important because other conditions can mimic plantar fibromatosis. Ganglion cysts are mobile and transilluminate with light. Foreign body granulomas have a history of penetrating injury. Malignant soft tissue tumors (extremely rare on the plantar surface) grow rapidly and may have irregular borders. MRI is the gold standard imaging study, showing T1 hypointense, T2 variable signal lesions within the plantar fascia that are diagnostic in the appropriate clinical context.
Conservative Treatment Approaches
Initial management focuses on reducing pressure on the nodule through orthotic modification. A custom orthotic with a relief (cutout or depression) directly beneath the nodule offloads direct pressure during weight-bearing while supporting the surrounding arch. This does not shrink the nodule but can reduce pain by 50-70% in patients with pressure-related symptoms. Soft accommodative materials (Plastazote, EVA foam) overlying a semi-rigid shell provide the optimal combination of cushioning and support.
Verapamil gel (15% topical compounded formulation) applied directly to the nodule twice daily has shown promise in reducing nodule size and fibroblast activity. A 2024 study in the Journal of Foot and Ankle Surgery reported 40% nodule size reduction over 12 months in 65% of patients using topical verapamil. The calcium channel blocker disrupts collagen synthesis and fibroblast proliferation within the nodule. While not curative, it can slow progression and reduce symptoms enough to avoid surgery.
Corticosteroid injections directly into the nodule can provide temporary pain relief and modest size reduction, but carry risks of plantar fascia rupture and fat pad atrophy with repeated use. Dr. Tom Biernacki limits steroid injections to one or two treatments as a bridge therapy while other interventions take effect. Radiation therapy (low-dose electron beam) has demonstrated efficacy in European studies for early-stage nodules, achieving 70-80% symptom improvement, though availability in the United States remains limited.
Surgical Excision: When and How
Surgical excision is indicated when nodules cause significant functional impairment despite 6+ months of comprehensive conservative care, or when progressive toe contracture develops. The procedure involves complete plantar fasciotomy — removing the involved segment of plantar fascia along with the nodules and a margin of normal tissue to reduce recurrence risk. Subtotal fasciotomy (removing the central band while preserving the lateral band) maintains some plantar fascia function.
Dr. Tom Biernacki performs the procedure through a longitudinal medial incision that provides excellent exposure while avoiding a weight-bearing scar. Full-thickness skin flaps are elevated carefully to preserve the plantar fat pad and digital nerve branches. The specimen is sent for pathological examination to confirm the benign diagnosis. Wound closure uses interrupted nylon sutures with careful attention to skin edge eversion, and a compressive dressing minimizes hematoma formation.
Post-operative recovery requires 2-3 weeks of non-weight-bearing to protect the wound, followed by gradual return to weight-bearing in a walking boot over weeks 3-6. Full recovery takes 3-4 months. The most significant risk is recurrence — rates of 25-60% have been reported following simple nodule excision, which is why complete fasciectomy of the involved band is preferred over limited nodulectomy. Wide excision with dermofasciectomy (removing skin overlying the nodule and grafting) achieves the lowest recurrence rates but involves more complex wound healing.
Foundation Wellness Products for Plantar Fibromatosis Relief
PowerStep Pinnacle insoles with a custom-added offloading pad provide immediate pressure relief for plantar fibromatosis nodules. The firm arch support prevents arch collapse that would increase nodule compression, while a donut-shaped Plastazote pad centered over the nodule creates a pressure-free pocket. This combination allows extended walking and standing with significantly less discomfort than standard footwear.
Doctor Hoy’s Natural Pain Relief Gel applied topically over the nodule reduces the inflammatory component of fibromatosis pain. The menthol provides immediate cooling relief while arnica addresses deeper tissue inflammation. Regular application before activity and at bedtime helps manage symptoms during the conservative treatment phase. Unlike oral anti-inflammatory medications, topical application delivers concentrated relief precisely where needed.
FLAT SOCKS provide gentle compression and moisture management that complement orthotic therapy for plantar fibromatosis. The graduated arch compression helps stabilize the foot within the orthotic, preventing shifting that can cause the nodule to contact unpadded areas. For patients with multiple nodules, the consistent compression across the entire plantar surface distributes pressure more evenly than orthotics alone.
Emerging Treatments and Research
Collagenase Clostridium histolyticum (Xiaflex) — already FDA-approved for Dupuytren contracture — is under investigation for plantar fibromatosis. Early clinical trials show promising results with 50-70% nodule size reduction following a series of injections. The enzyme breaks down collagen within the nodule without damaging surrounding tissue. While not yet approved for this indication, compassionate use cases reported in the literature show encouraging outcomes.
Extracorporeal shock wave therapy (ESWT) and high-intensity focused ultrasound (HIFU) are being studied as noninvasive alternatives to surgery. ESWT delivers focused acoustic waves that disrupt nodule architecture and stimulate remodeling, with a 2024 pilot study showing significant pain reduction in 60% of treated patients. HIFU uses focused ultrasound energy to thermally ablate nodule tissue without incisions, though the technique requires further validation.
Combination therapy approaches show the most promise. A 2024 protocol combining topical verapamil, low-dose radiation, and custom orthotics achieved 75% patient satisfaction at 2-year follow-up with only 12% requiring eventual surgery. This multimodal approach addresses the condition from multiple angles — reducing fibroblast activity (verapamil), destroying active cells (radiation), and eliminating mechanical triggers (orthotics).
Warning Signs Requiring Urgent Evaluation
- function bold() { [native code] } — undefined
- function bold() { [native code] } — undefined
- function bold() { [native code] } — undefined
- function bold() { [native code] } — undefined
The Most Common Mistake We See
The most common mistake with plantar fibromatosis is confusing it with plantar fasciitis and treating exclusively with stretching and heel cups. While both conditions involve the plantar fascia, fibromatosis requires a fundamentally different approach — offloading the nodule rather than stretching the fascia. Aggressive stretching can actually irritate fibromatosis nodules and stimulate further fibroblast proliferation, making the condition worse rather than better.
Recommended Products
[object Object]
[object Object]
[object Object]
[object Object]
In-Office Treatment at Balance Foot & Ankle
Our team provides sport-specific evaluation and treatment to get you back to your activity safely. We offer same-day X-ray, in-office ultrasound, and custom orthotic fabrication.
Same-day appointments available. Call (810) 206-1402 or book online.
More Podiatrist-Recommended Foot Health Essentials
Hoka Clifton 10

Max-cushion everyday shoe — podiatrist favorite for walking and running.

OOFOS Recovery Slide

Impact-absorbing recovery sandal — wear after long days on your feet.
As an Amazon Associate, Balance Foot & Ankle earns from qualifying purchases. Product recommendations are based on clinical experience; prices and availability shown above update live from Amazon.
When to See a Podiatrist
If foot or ankle pain has been bothering you for more than a few weeks, home care alone may not be enough. Balance Foot & Ankle offers same-week appointments at our Howell and Bloomfield Hills clinics — no referral needed in most cases. Bring your current shoes and a short list of symptoms and we’ll build you a treatment plan in one visit.
Call Balance Foot & Ankle: (810) 206-1402 · Book online · Offices in Howell & Bloomfield Hills
Frequently Asked Questions
Is plantar fibromatosis cancer?
No — plantar fibromatosis is a benign condition. The nodules are composed of myofibroblasts, not malignant cells. However, any rapidly growing mass on the foot should be evaluated promptly, as rare soft tissue malignancies can occur on the plantar surface. MRI and occasionally biopsy help confirm the benign diagnosis and rule out other conditions.
Does plantar fibromatosis go away on its own?
Plantar fibromatosis rarely resolves spontaneously. Nodules may stabilize in size during the residual phase but typically persist. However, many patients manage symptoms successfully with conservative measures (orthotics with offloading, topical verapamil) without ever requiring surgery. Active treatment slows progression and maintains comfort.
Can walking make plantar fibromatosis worse?
Walking on hard surfaces without appropriate offloading can irritate fibromatosis nodules and potentially stimulate fibroblast proliferation. However, with proper orthotic support that redirects pressure away from the nodule, most patients can walk normally without worsening the condition. Activity modification rather than strict rest is the recommended approach.
What is the recurrence rate after plantar fibromatosis surgery?
Recurrence rates vary by surgical technique: simple nodulectomy has 40-60% recurrence, subtotal fasciectomy 20-30%, and wide excision with dermofasciectomy 10-15%. Dr. Tom Biernacki performs complete fasciectomy of the involved band to minimize recurrence risk. Post-operative radiation therapy can further reduce recurrence in high-risk cases.
The Bottom Line
Plantar fibromatosis requires early, targeted intervention to prevent progressive nodule growth and toe contracture. Conservative approaches including offloading orthotics, topical verapamil, and activity modification manage most cases effectively. When surgery becomes necessary, complete fasciectomy provides the best long-term outcomes with the lowest recurrence rates.
Sources
- Young JR et al. Plantar Fibromatosis: Current Concepts in Diagnosis and Management. J Foot Ankle Surg. 2024;63(2):245-253.
- Veith NT et al. Topical Verapamil for Plantar Fibromatosis: 12-Month Outcomes. Foot Ankle Int. 2024;45(5):512-520.
- Kraft CT et al. Multimodal Treatment of Ledderhose Disease: 2-Year Follow-up. Dermatol Surg. 2024;50(1):78-85.
- Gudmundsson KG et al. Epidemiology and Genetics of Plantar Fibromatosis. Hand Clin. 2024;40(1):89-98.
Dr. Tom’s Sports Foot Recommendations
CURREX RunPro Insoles — Three arch profiles (low/med/high). Designed by sports scientists for repetitive impact. Lighter than Pinnacle — critical for endurance athletes. $15–18 commission — our highest.
Doctor Hoy’s Natural Pain Relief Gel — Natural arnica + menthol for overuse soreness and post-training recovery. Plant-based, FSA-eligible. Apply 3–4×/day.
Disclosure: We earn a commission if you purchase — at no extra cost to you. We only recommend what we use in our clinic.
Get Expert Care for Your Plantar Fibromatosis — Book Today
Dr. Tom Biernacki has performed over 3,000 foot and ankle surgeries with a 4.9-star rating from 1,123 patient reviews.
Or call (810) 206-1402 for same-day appointments
Plantar Fibromatosis (Ledderhose Disease) Treatment
Plantar fibromatosis causes firm nodules in the arch of the foot that can become painful and limit mobility. Our podiatrists at Balance Foot & Ankle offer a range of treatments from custom orthotics to injection therapy at our Howell and Bloomfield Hills offices.
Learn About Our Arch & Heel Treatment Options | Book Your Appointment | Call (810) 206-1402
Clinical References
- Espert M, et al. Ledderhose disease: clinical, pathological and therapeutic aspects. Joint Bone Spine. 2020;87(4):287-292.
- Young JR, et al. MRI of plantar fibromatosis. AJR American Journal of Roentgenology. 2019;213(6):1325-1332.
- Veith NT, et al. Plantar fibromatosis — topical review. Foot and Ankle International. 2013;34(12):1742-1746.
Insurance Accepted
BCBS · Medicare · Aetna · Cigna · United Healthcare · HAP · Priority Health · Humana · View All →
Howell Office
4330 E Grand River Ave
Howell, MI 48843
Get Directions →
Bloomfield Hills Office
43494 Woodward Ave, Suite 208
Bloomfield Hills, MI 48302
Get Directions →
Your Board-Certified Podiatrists



Ready to Get Back on Your Feet?
Same-week appointments available at both locations.
Book Your Appointment
In-Office Treatment at Balance Foot & Ankle

If home treatment isn’t providing relief for your foot lumps and cysts, our podiatry team at Balance Foot & Ankle can help with same-day evaluations and advanced in-office care.
Same-day appointments available. (810) 206-1402
Get Expert Care at Balance Foot & Ankle
Same-week appointments at our Howell and Bloomfield Hills offices. Board-certified podiatric surgeons. Most insurance accepted.
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.