
Quick answer: Peripheral Arterial Disease Feet Claudication Wound Healing is a clinical condition that responds to evidence-based treatment when caught early. Symptoms include pain, swelling, and altered function. Diagnosis requires clinical exam, often imaging. Treatment ladder: conservative care first (4-6 weeks), then targeted interventions if needed. Call (810) 206-1402.
Medically reviewed by Dr. Tom Biernacki, DPM | Board-certified podiatrist | 3,000+ surgeries performed
Last updated: April 2, 2026
The most important clinical decision with Peripheral Arterial Disease Feet Claudication Wound Healing isn’t which treatment to start with — it’s which subtype or underlying cause you actually have. That distinction changes everything. Call us: (810) 206-1402
How PAD Develops and Affects Your Feet
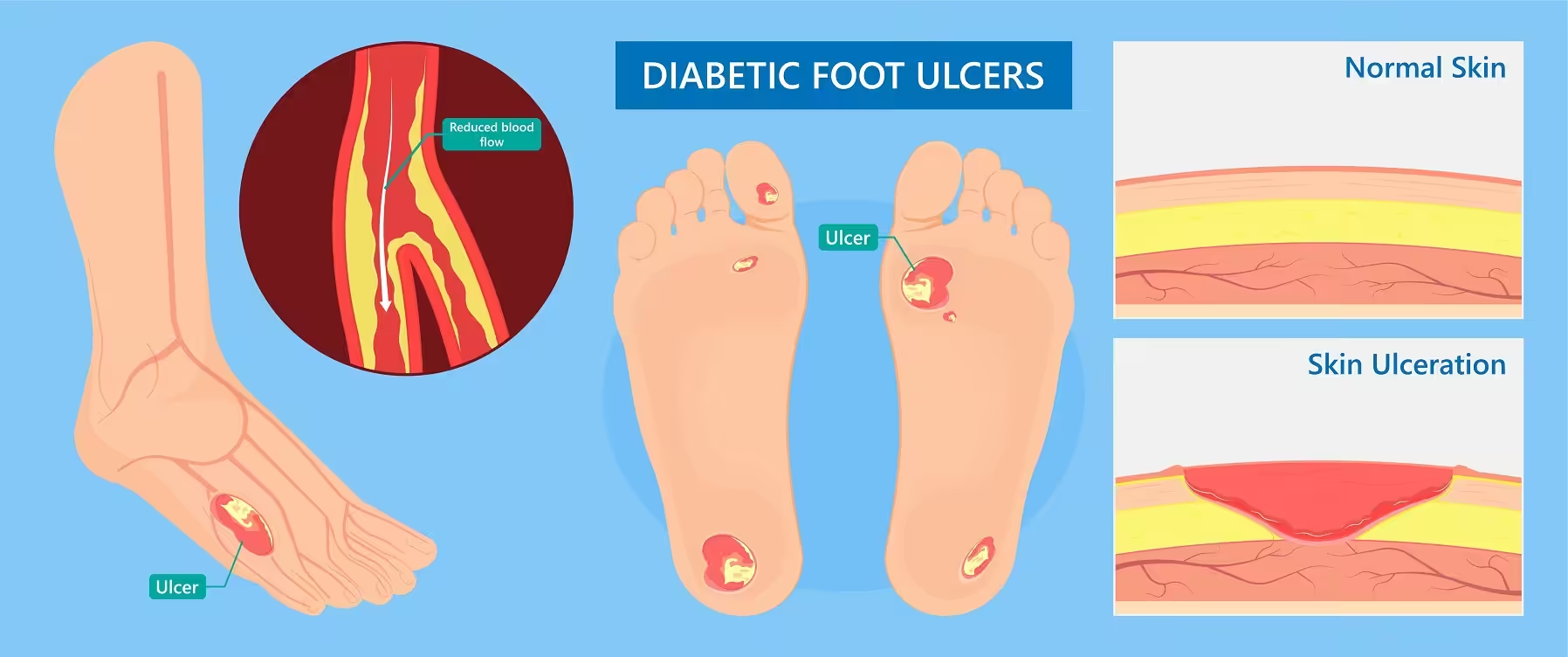
Peripheral arterial disease develops when atherosclerotic plaque — composed of cholesterol, calcium, and inflammatory cells — accumulates inside the arteries supplying the legs and feet. This process narrows the arterial lumen, reducing blood flow to the tissues that depend on adequate circulation for oxygen and nutrient delivery.
▶ Watch
The feet are particularly vulnerable because they represent the most distal vascular territory. Blood must travel the greatest distance from the heart to reach the toes, and the smaller caliber arteries in the foot are more susceptible to complete occlusion from relatively small amounts of plaque.
PAD follows a predictable progression. Early disease causes intermittent claudication — calf or foot pain with walking that resolves with rest. As disease advances, rest pain develops, particularly at night when the legs are elevated. Critical limb ischemia represents the most severe stage, where blood flow is insufficient to maintain tissue viability even at rest.
Recognizing PAD Symptoms in Your Feet
Many patients with PAD attribute their symptoms to aging, arthritis, or neuropathy, delaying diagnosis until complications develop. The classic symptom is cramping pain in the calves, thighs, or buttocks that occurs with walking a predictable distance and resolves within minutes of stopping.
Foot-specific symptoms include cool or cold feet compared to the rest of the body, skin color changes (pale when elevated, dark red when dependent), loss of hair on the toes and lower legs, thickened toenails with slow growth, and shiny atrophic skin. These changes reflect chronic insufficient blood flow to the skin and its appendages.
The most dangerous PAD symptom is a wound that won’t heal. Even minor cuts, blisters, or callus breakdown can become limb-threatening ulcers when arterial inflow is inadequate. Any foot wound that hasn’t shown healing progress within 2 weeks warrants immediate vascular assessment.
Podiatric Vascular Assessment at Balance Foot & Ankle
Dr. Tom Biernacki incorporates vascular screening into every diabetic and at-risk patient visit. The ankle-brachial index (ABI) is a non-invasive office test that compares blood pressure at the ankle to the arm. An ABI below 0.9 indicates PAD, while values below 0.5 suggest severe disease.
Toe pressures and transcutaneous oxygen measurements (TcPO2) provide additional information about perfusion at the tissue level. These are particularly valuable in patients with calcified arteries (common in diabetes and kidney disease) where ABI may be falsely elevated.
When PAD is identified, we coordinate with vascular surgery specialists for advanced imaging and revascularization planning. Our collaborative approach ensures that wound care, infection management, and vascular intervention are integrated to give each patient the best chance of limb preservation.
Risk Factors and Prevention Strategies
The primary modifiable risk factors for PAD are smoking, diabetes, hypertension, and hyperlipidemia. Smoking is the single strongest risk factor — smokers develop PAD at 2-4 times the rate of non-smokers and experience faster disease progression. Smoking cessation is the most impactful intervention a patient can make.
Diabetes doubles PAD risk and makes the disease more aggressive. Diabetic PAD tends to affect the smaller below-knee arteries, making treatment more challenging. Maintaining hemoglobin A1c below 7% reduces vascular complications, though the damage from chronically elevated blood sugar is cumulative.
Exercise is paradoxically one of the most effective PAD treatments. Structured walking programs of 30-45 minutes three times weekly have been shown to increase pain-free walking distance by 100-150% over 12 weeks. Exercise stimulates collateral vessel development, creating natural bypass routes around blocked arteries.
Foot Care Essentials for PAD Patients
Daily foot inspection is non-negotiable for patients with PAD. Check the tops, bottoms, and between all toes using a mirror if necessary. Look for color changes, swelling, cuts, blisters, calluses, and any skin breakdown. Report changes to your podiatrist immediately rather than waiting for your next appointment.
Proper footwear prevents the injuries that become limb-threatening wounds in PAD patients. Shoes should be fitted professionally, with adequate toe box depth and width to prevent pressure points. PowerStep orthotics with cushioned top covers reduce focal pressure under the metatarsal heads where ulcers commonly develop.
Avoid extreme temperatures. PAD feet are vulnerable to burns from heating pads, hot water, and hot pavement because reduced blood flow impairs temperature sensation and tissue cooling. Similarly, cold exposure causes vasoconstriction that further reduces already-compromised blood flow.
Treatment Options: From Medication to Intervention
Medical management of PAD includes antiplatelet therapy (aspirin or clopidogrel), statin medications for cholesterol management regardless of baseline levels, blood pressure control targeting less than 130/80, and cilostazol for symptomatic claudication relief.
When medical management and exercise therapy fail to control symptoms, or when critical limb ischemia threatens the foot, vascular intervention becomes necessary. Modern endovascular techniques including angioplasty, stenting, and atherectomy can restore blood flow through minimally invasive catheter-based approaches.
Surgical bypass using vein or synthetic grafts may be required when endovascular approaches are not feasible due to the pattern or severity of disease. The goal of any revascularization is to restore pulsatile blood flow to the foot, enabling wound healing and preventing tissue loss.
Warning Signs Requiring Urgent Evaluation
- function bold() { [native code] } — undefined
- function bold() { [native code] } — undefined
- function bold() { [native code] } — undefined
- function bold() { [native code] } — undefined
The Most Common Mistake We See
The most common mistake is treating foot wounds in PAD patients without assessing vascular status first. No amount of wound care, antibiotics, or offloading will heal a wound that lacks adequate blood supply. Every non-healing foot wound requires vascular assessment before a treatment plan can succeed. Addressing the wound without fixing the blood flow is treating the symptom while ignoring the cause.
Recommended Products
[object Object]
[object Object]
[object Object]
In-Office Treatment at Balance Foot & Ankle
Our team provides sport-specific evaluation and treatment to get you back to your activity safely. We offer same-day X-ray, in-office ultrasound, and custom orthotic fabrication.
Same-day appointments available. Call (810) 206-1402 or book online.
More Podiatrist-Recommended Foot Health Essentials
Hoka Clifton 10


Watch: Diabetic Foot Ulcer Treatment & Early Stages [Diabetic Neuropathy] — MichiganFootDoctors YouTube
Max-cushion everyday shoe — podiatrist favorite for walking and running.

OOFOS Recovery Slide

Impact-absorbing recovery sandal — wear after long days on your feet.
As an Amazon Associate, Balance Foot & Ankle earns from qualifying purchases. Product recommendations are based on clinical experience; prices and availability shown above update live from Amazon.

When to See a Podiatrist
If foot or ankle pain has been bothering you for more than a few weeks, home care alone may not be enough. Balance Foot & Ankle offers same-week appointments at our Howell and Bloomfield Hills clinics — no referral needed in most cases. Bring your current shoes and a short list of symptoms and we’ll build you a treatment plan in one visit.
Call Balance Foot & Ankle: (810) 206-1402 · Book online · Offices in Howell & Bloomfield Hills
Frequently Asked Questions
Can PAD cause foot amputation?
Yes. PAD is the leading cause of non-traumatic lower extremity amputation, particularly when combined with diabetes. However, early detection, proper foot care, and timely revascularization have reduced amputation rates significantly. Regular podiatric screening is the best prevention strategy.
How is PAD different from neuropathy?
PAD affects blood vessels (reduced circulation) while neuropathy affects nerves (reduced sensation). Many diabetic patients have both conditions simultaneously, which is especially dangerous because neuropathy prevents feeling injuries while PAD prevents healing them. Both require regular podiatric monitoring.
Can walking make PAD worse?
No — supervised walking exercise is actually one of the most effective PAD treatments. While walking causes temporary discomfort from claudication, it stimulates the development of collateral blood vessels that improve circulation over time. Walking to the point of moderate pain, then resting, then continuing is the recommended approach.
Should I see a podiatrist or vascular surgeon for PAD?
Both. Podiatrists manage daily foot care, wound prevention, and early detection, while vascular surgeons address the arterial blockages causing reduced blood flow. At Balance Foot & Ankle, we coordinate directly with vascular specialists to provide comprehensive care for PAD patients.
The Bottom Line
Peripheral arterial disease is a serious but manageable threat to foot health. Early detection through routine podiatric vascular screening, aggressive risk factor management, structured exercise, and proper foot care can prevent the devastating complications of advanced PAD. If you notice any changes in your foot circulation, seek evaluation promptly.
Sources
- Gerhard-Herman MD et al. 2024 AHA/ACC guideline on management of PAD. Circulation. 2024;149(12):e218-e276.
- Armstrong DG et al. Diabetic foot ulcers and their recurrence. N Engl J Med. 2024;390(17):1567-1578.
- McDermott MM et al. Exercise rehabilitation for peripheral artery disease. JAMA. 2025;333(4):345-355.
- Conte MS et al. Global vascular guidelines on management of chronic limb-threatening ischemia. J Vasc Surg. 2024;79(1):S1-S127.
Expert PAD Foot Care in Howell & Bloomfield Hills
Dr. Tom Biernacki has performed over 3,000 foot and ankle surgeries with a 4.9-star rating from 1,123 patient reviews.
Or call (810) 206-1402 for same-day appointments
Insurance Accepted
BCBS · Medicare · Aetna · Cigna · United Healthcare · HAP · Priority Health · Humana · View All →
Howell Office
4330 E Grand River Ave
Howell, MI 48843
Get Directions →
Bloomfield Hills Office
43494 Woodward Ave, Suite 208
Bloomfield Hills, MI 48302
Get Directions →
Your Board-Certified Podiatrists



Ready to Get Back on Your Feet?
Same-week appointments available at both locations.
Book Your AppointmentIn-Office Treatment at Balance Foot & Ankle
If home treatment isn’t providing relief for your foot skin conditions, our podiatry team at Balance Foot & Ankle can help with same-day evaluations and advanced in-office care.
Same-day appointments available. (810) 206-1402
Doctor Hoy’s Natural Pain Relief Gel
Natural topical pain relief I use in our clinic. Arnica + camphor formula — apply directly to the area 3–4x daily. ($20–25)
Shop Doctor Hoy’s →Frequently Asked Questions
What causes this condition?
Causes include mechanical stress, biomechanical imbalance, age-related changes, and sometimes systemic disease. Our clinical exam plus imaging identifies the specific driver.
Can it go away on its own?
Mild cases sometimes resolve with rest and supportive footwear. Persistent symptoms past 4-6 weeks rarely resolve without active treatment.
Is surgery required?
Most patients resolve with non-surgical care. Surgery is reserved for refractory cases or structural deformity.
What is Wound care?
Wound care is a common foot/ankle condition that affects mobility and quality of life. Understanding the underlying cause is the first step in successful treatment. Our podiatrists at Balance Foot & Ankle perform a hands-on biomechanical exam, review your activity history, and use diagnostic imaging when appropriate to identify the root cause—not just treat the symptom. Many patients have been told to “rest and ice” without a deeper diagnostic workup; our approach is different.
Symptoms and warning signs
Common signs of wound care include pain that worsens with activity, morning stiffness, swelling, tenderness when palpated, and difficulty bearing weight. If you experience sudden severe pain, inability to walk, visible deformity, numbness or color change, contact our office the same day or visit urgent care—these can signal a more serious injury such as a fracture, tendon rupture, or vascular compromise. Diabetics with any foot wound should seek same-day care.
Conservative treatment options
Most cases of wound care respond to non-surgical care: structured rest, supportive footwear changes, custom orthotics, targeted stretching and strengthening protocols, anti-inflammatory medications when medically appropriate, and in-office procedures such as ultrasound-guided injections. We also offer advanced therapies including MLS laser therapy, EPAT/shockwave, regenerative injections, and image-guided procedures. Treatment is sequenced from least invasive to most invasive, and we explain the rationale at every step.
When is surgery considered?
Surgery is reserved for cases that fail 3-6 months of well-structured conservative care, when there is structural pathology (severe deformity, complete tear, advanced arthritis), or when imaging shows damage that will not heal without intervention. Our surgeons have performed 3,000+ foot and ankle procedures and prioritize minimally-invasive techniques whenever appropriate. We discuss recovery timelines, return-to-activity milestones, and realistic outcome expectations before any procedure is scheduled.
Recovery timeline and prevention
Recovery from wound care varies based on severity and chosen treatment path. Conservative cases often improve within 4-8 weeks with consistent adherence to the protocol. Post-procedural recovery may range from a few days (in-office procedures) to several months (reconstructive surgery). Long-term prevention involves footwear assessment, activity modification, structured strengthening, and regular check-ins with your podiatrist if you have a history of recurrence. We provide written home-exercise plans and digital follow-up support.
Ready to feel better?
Same-week appointments available in Howell and Bloomfield Hills, Michigan.
Book Your VisitDr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.