

| Home Remedy | Active Agent | Evidence Level | Antifungal Mechanism | Realistic Cure Rate |
|---|---|---|---|---|
| Tea tree oil (Melaleuca) | Terpinen-4-ol; alpha-terpineol | Low-moderate (small studies) | Disrupts fungal cell membrane | ~18% mycological cure; best for surface discoloration |
| Vicks VapoRub | Thymol; camphor; eucalyptol | Low (one small study) | Thymol has antifungal properties; subungual penetration poor | ~28% in single study; not replicated |
| Diluted bleach foot soak | Sodium hypochlorite | Low | Oxidative damage to fungal cells | Insufficient data; can irritate/dry skin; low penetration |
| Apple cider vinegar | Acetic acid | Very low (anecdotal) | Mild acidification may inhibit fungal growth on skin surface | No clinical evidence of nail cure |
| Hydrogen peroxide soak | H₂O₂ 3% | Very low | Oxidative; insufficient nail penetration | No clinical evidence of nail cure |
| Coconut oil | Caprylic acid; lauric acid | Very low (in vitro only) | In-lab antifungal; no evidence of nail penetration in humans | No clinical evidence |
| OTC topical antifungal (clotrimazole/tolnaftate) | Imidazole / thiocarbamate | Low for nails (moderate for skin) | Ergosterol synthesis inhibition | Effective for athlete’s foot (skin); minimal nail penetration |
| Treatment Option | Type | Cure Rate (mycological) | Duration | Best Candidate |
|---|---|---|---|---|
| Oral terbinafine (Lamisil) | Prescription systemic antifungal | 70–80% | 12 weeks (fingernails); 16 weeks (toenails) | Moderate-to-severe onychomycosis; healthy liver function |
| Oral itraconazole (pulse dosing) | Prescription systemic antifungal | 55–65% | 3 pulse courses (1 week on, 3 weeks off) | Patients who cannot take terbinafine; multiple drug interactions possible |
| Efinaconazole 10% (Jublia) | Prescription topical antifungal | 17–18% complete cure; 55% mycological cure | 48 weeks daily application | Mild-moderate onychomycosis; contraindication to oral therapy |
| Ciclopirox nail lacquer (Penlac) | Prescription topical antifungal | 6–12% complete cure | Up to 48 weeks | Mild distal-lateral subungual onychomycosis only |
| Laser therapy (Nd:YAG 1064nm) | In-office device | Variable: 30–60% in studies; no FDA-approved cure claim | 3–4 sessions over 3 months | Patients preferring no systemic medication; adjunct to topical |
| Nail avulsion + antifungal | Podiatric procedure + medication | Higher than topical alone | Immediate + medication course | Severely thickened, painful, or non-responsive nails |
Toenail fungus home remedies — Vicks VapoRub, tea tree oil, vinegar — work for some early-stage cases and do nothing for advanced ones. Recognizing when to escalate to medical treatment matters.
Related Conditions
In This Article
- What home remedy actually cures toenail fungus?
- What Is Toenail Fungus
- 7 Evidence-Based Home Remedies for Toenail Fungus
- How to Apply Home Remedies Correctly
- What Doesn’t Work — Common Mistakes
- Over-the-Counter Antifungal Options
- Prevention Strategies That Actually Work
- Red Flags — When Home Remedies Are Not Enough
- Recommended Products for Toenail Fungus
- In-Office Treatment at Balance Foot & Ankle
- Frequently Asked Questions
- Sources
You’re in the right place. Dr. Tom Biernacki, DPM, FACFAS — board-certified foot & ankle surgeon with 3,000+ surgeries — explains exactly what toenail fungus home remedies means and what works. Call (810) 206-1402 for same-day appointment at Howell or Bloomfield Hills.
![Tea Tree Oil Toenail Fungus Home Treatment [Doctor Cure!]](https://www.michiganfootdoctors.com/wp-content/cache/flying-press/a434e04a532dc4826563b11aa0541dd4.jpg)
Watch: Tea Tree Oil Toenail Fungus Home Treatment [Doctor Cure!] — MichiganFootDoctors YouTube
Foot pain isn't resolving?
Same-week appointments at Howell & Bloomfield Hills
The most effective toenail fungus home remedies are topical tea tree oil (applied twice daily), white vinegar foot soaks (1:2 vinegar-to-water, 20 minutes daily), and hydrogen peroxide soaks (3% solution). These reduce surface fungal load but rarely eliminate deep nail plate infection. Mild cases may clear in 3–6 months; severe or spreading fungus needs prescription treatment.
You’ve noticed it for weeks — a toenail that’s turned yellowish or brownish, thicker than normal, and starting to crumble at the edge. You’ve tried scrubbing it harder, keeping it trimmed, maybe even bought an antifungal spray. But it keeps spreading. You’re not alone: onychomycosis (toenail fungus) affects roughly 14% of the general population and up to 50% of adults over 70. In our clinic, we see it weekly — and we also see the mistakes people make treating it at home that delay real resolution by months.
The honest truth is that home remedies for toenail fungus have real limitations. They’re effective at controlling surface fungal colonies but struggle to penetrate the nail plate to eliminate deep infection. That said, for mild-to-moderate cases caught early, the right home approach used consistently can produce visible improvement. Here’s exactly what works, what doesn’t, and when you need to escalate.
What Is Toenail Fungus
Toenail fungus (onychomycosis) is a fungal infection of the nail plate, nail bed, or both. The most common cause is dermatophytes — primarily Trichophyton rubrum — which feed on keratin, the protein that makes up your nails. Less commonly, non-dermatophyte molds and yeasts (like Candida) cause nail infections, which behave somewhat differently and may not respond to the same treatments.
The infection usually starts at the free edge or sides of the nail and slowly progresses toward the cuticle. As fungi digest the keratin, the nail thickens, discolors (yellow, brown, white, or black), becomes brittle, and may separate from the nail bed (onycholysis). In severe cases the entire nail plate is involved and secondary bacterial infection becomes a concern, especially in diabetic patients.
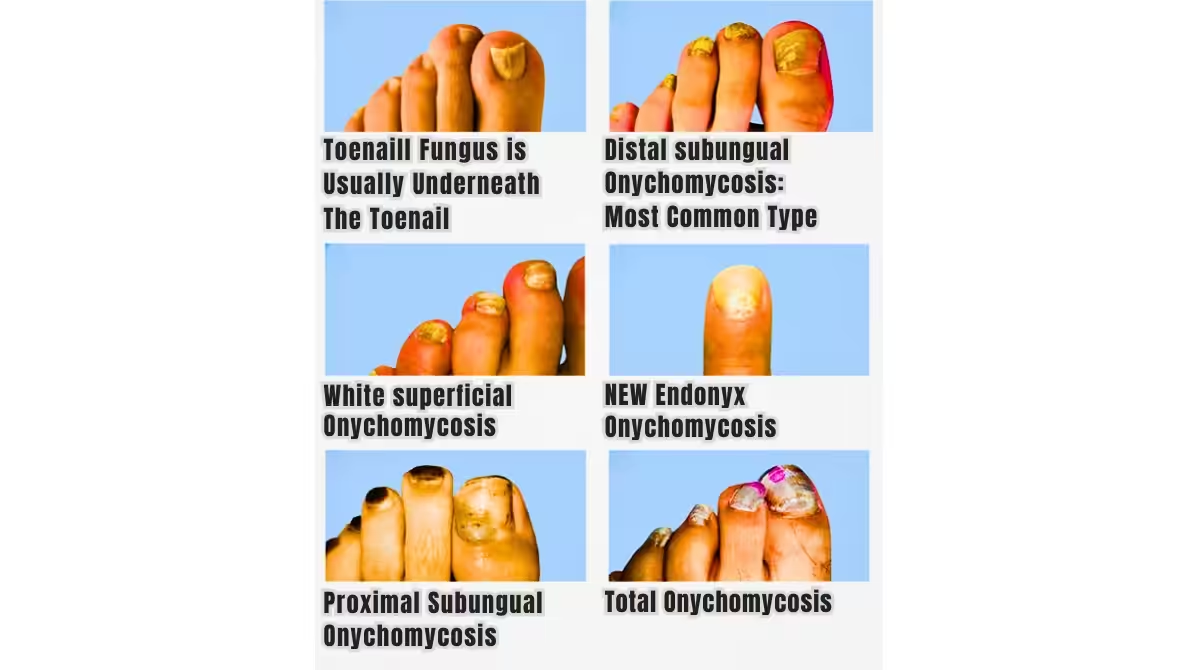
| Type | Where It Starts | Common Organism | Home Remedy Success Rate |
|---|---|---|---|
| Distal Subungual (most common) | Free nail edge | T. rubrum | Moderate (early) |
| White Superficial | Nail surface (chalky white) | T. mentagrophytes | Good — most responsive |
| Proximal Subungual | Near cuticle | Dermatophytes | Poor — needs Rx |
| Total Dystrophic | Entire nail | Mixed | Very poor — needs Rx |
7 Evidence-Based Home Remedies for Toenail Fungus
Not all home remedies are equal. These seven have at least some scientific support, ranging from controlled clinical trials to well-documented antifungal mechanisms. Ranking them from most to least evidence:
1. Tea Tree Oil (Melaleuca Oil)
Tea tree oil is the most studied topical home remedy for nail fungus. It contains terpinen-4-ol, which disrupts fungal cell membranes. A 1999 randomized controlled trial in the Journal of Family Practice found that 100% tea tree oil applied twice daily produced partial or full resolution in 18% of subjects versus 11% for clotrimazole cream — comparable but not superior to OTC antifungals. Application must be consistent for at least 6 months. Use 100% pure tea tree oil (not diluted blends); apply with a cotton swab directly to and under the free edge of the nail twice daily. In our clinic, we recommend tea tree oil as an adjunct to prescription treatment, not a standalone for moderate-to-severe cases.
2. White Vinegar Foot Soaks
Vinegar creates an acidic environment (pH 2.5–3.5) that inhibits fungal growth. Mix one part white vinegar with two parts warm water and soak the affected foot for 15–20 minutes daily. A small 2017 study found that acetic acid at this concentration demonstrated antifungal activity against T. rubrum in vitro. While clinical trial data is limited, the safety profile is excellent and many patients report improvement in nail color and texture with consistent daily use over 3–4 months. Dry thoroughly afterward — moisture between toes promotes fungal regrowth.
3. Hydrogen Peroxide Soaks
A 3% hydrogen peroxide solution (standard drugstore concentration) can be applied directly to the nail or used as a foot soak. Hydrogen peroxide is an oxidizing agent that kills fungi by releasing oxygen radicals. Soak affected nails for 10–15 minutes daily, or apply with a cotton ball twice daily. Some protocols combine hydrogen peroxide with white vinegar (apply one, let dry, then the other — never mix them together as they form peracetic acid). This approach is most useful for superficial white onychomycosis where the surface layer is accessible.
4. Vicks VapoRub
This one surprises patients. Vicks VapoRub contains thymol, eucalyptus oil, and camphor — all with documented antifungal properties. A 2011 study in the Journal of the American Board of Family Medicine found that 83% of patients using Vicks VapoRub daily showed improvement at 48 weeks, with 27.8% achieving complete cure. Apply a thin layer to the nail nightly and cover with a cotton sock. This is particularly suitable for patients who can’t tolerate daily soaks. The catch: it’s slow — expect 6–12 months of nightly application before seeing full results.
5. Baking Soda
Baking soda (sodium bicarbonate) raises the local pH, creating an environment fungal spores find inhospitable. Make a paste with water and apply directly to the nail for 10–15 minutes before rinsing, or add ½ cup to a foot soak. Baking soda won’t cure an established infection but works well as a preventive measure and to reduce the spread of active infection to adjacent nails. It also absorbs odor-causing bacteria.
6. Oregano Oil
Oregano oil contains thymol and carvacrol, both potent antifungals in lab settings. Dilute to 1% concentration in a carrier oil (coconut or olive oil) before applying — undiluted oregano oil causes significant skin irritation. Apply with a cotton swab twice daily. The evidence base is primarily in vitro; clinical trials specific to nail fungus are limited. Tea tree oil has better supporting data, but oregano oil can be used in combination.
7. Proper Nail Trimming and Filing
This is often overlooked but mechanically important. Reducing nail thickness with a nail file removes infected keratin layers and allows topical agents to penetrate more deeply. Always use a dedicated nail file for the infected nail (never share it with uninfected nails), and discard it monthly. Trim the nail straight across as short as you can tolerate without causing pain. This isn’t a cure on its own, but it meaningfully increases the effectiveness of every topical remedy you apply afterward. In our clinic, we sometimes perform nail debridement — professional thinning — to maximize topical penetration in stubborn cases.
How to Apply Home Remedies Correctly
Consistency and preparation determine whether home remedies work. The biggest reason they fail is inconsistent application — most people stop at 2 months when they don’t see dramatic results, not realizing that the new nail growth needed to show clear, healthy nail takes 9–12 months of steady growth. Here’s the correct protocol:
Morning routine (5 minutes): After showering, dry feet thoroughly — including between toes — with a clean towel. Apply your chosen topical remedy (tea tree oil, vinegar soak, or hydrogen peroxide). Let it air-dry completely before putting on socks. Moisture trapping is the enemy.
Evening routine (5 minutes): Repeat application after evening hygiene. If using Vicks VapoRub, apply before bed and cover with cotton socks overnight. Trim and file once weekly using a dedicated implement.
Footwear hygiene: Spray the inside of your shoes daily with an antifungal foot spray. Rotate shoes so each pair dries completely between wearings. Wear moisture-wicking socks (not cotton, which holds moisture). In shared spaces (locker rooms, pools), always wear shower sandals.
What Doesn’t Work — Common Mistakes
The most common mistake we see is patients treating the symptom (discoloration) without addressing the cause (fungal load in the shoe environment). You can eliminate the nail fungus successfully, then immediately re-infect from contaminated shoes or socks. Treating the nail without decontaminating footwear is one of the leading reasons home treatment “fails.”
What genuinely doesn’t work:
Bleach soaks: Despite widespread internet promotion, soaking in diluted bleach is too harsh for the skin and nail tissue, can cause chemical burns, and has no proven benefit over safer alternatives. Skip this one entirely.
Essential oil diffusers or oral essential oils: Topical application is what matters for nail fungus. Inhaling or ingesting essential oils provides no benefit to nail tissue.
Cutting the nail extremely short or picking at it: This causes pain, nail bed injury, and possible secondary bacterial infection without removing the fungus. Trim normally and file gently — don’t traumatize the tissue.
Stopping treatment when the nail looks better: The nail looks better before it IS better. The old fungal nail grows out; new healthy nail grows in from the root. Keep applying treatment until completely new nail has grown in — typically 9–12 months for a great toenail.
Over-the-Counter Antifungal Options
If home remedies aren’t producing results after 2–3 months, step up to an OTC antifungal before going to prescription. The two most effective OTC nail antifungals are undecylenic acid and tolnaftate. Both are FDA-recognized antifungals, though their nail penetration is limited compared to prescription lacquers.
| Product Type | Active Ingredient | How to Use | Timeframe |
|---|---|---|---|
| Nail lacquer (e.g., Fungi-Nail) | Undecylenic acid | Daily brush-on | 6–12 months |
| Antifungal cream/gel | Tolnaftate, clotrimazole | Twice daily to nail margins | 3–6 months |
| Antifungal spray | Miconazole | Daily to nail and shoe interior | Ongoing prevention |
| Prescription nail lacquer | Ciclopirox 8% (Penlac) | Daily lacquer, weekly remove | 48 weeks |
Prescription oral antifungals (terbinafine/Lamisil, itraconazole) are significantly more effective — cure rates of 60–80% vs. 10–30% for topicals — but require a prescription and come with potential liver side effects requiring monitoring. Discuss these with your podiatrist if topical treatment hasn’t worked after 6 months.
Prevention Strategies That Actually Work
In our clinic, we see a lot of successfully treated toenail fungus that came back within a year because the patient didn’t address the fungal reservoir in their environment. Here’s how to break the cycle for good:
Footwear hygiene: Use antifungal spray inside every shoe after each wear. Replace old athletic shoes (fungal spores survive in foam for months). Wear open-toed or well-ventilated shoes when possible. Alternate shoes daily so each pair dries completely.
Sock selection: Moisture-wicking synthetic or wool socks dramatically outperform cotton for fungal prevention. FLAT SOCKS no-show inserts work well for casual footwear where regular socks cause overheating.
Shower and pool hygiene: Wear shower sandals or flip-flops in public showers, locker rooms, and pool decks — these are the highest-risk environments for picking up dermatophytes. Avoid walking barefoot in shared spaces entirely.
Keep feet dry: Dry between every toe after bathing. Consider applying a light dusting of antifungal powder to feet and shoe interiors, especially in hot months or if you have hyperhidrosis (excessive sweating).
Don’t share: Never share nail clippers, files, or towels. If you get pedicures, bring your own instruments or verify the salon sterilizes tools between clients with an autoclave (not just UV light).
Nail care routine: Keep toenails trimmed short and straight across. Long nails trap moisture and debris underneath. Don’t round corners — straight cuts reduce ingrown risk.
Red Flags — When Home Remedies Are Not Enough
- You have diabetes — any nail abnormality requires professional evaluation; risk of secondary bacterial infection and ulceration
- The nail is painful, warm, or showing green/black discoloration — possible bacterial superinfection
- You have peripheral vascular disease or poor circulation — topical treatments may not penetrate adequately and infection risk is high
- The infection is spreading to multiple nails or skin (tinea pedis/athlete’s foot alongside nail fungus) — systemic treatment is needed
- No improvement after 6 months of consistent home treatment — you likely need prescription oral antifungal
- The nail is lifting, detaching, or the nail bed is visibly red/angry — onycholysis with secondary infection risk
Recommended Products for Toenail Fungus
FLAT SOCKS No-Show Inserts
FLAT SOCKS are no-sock shoe inserts made from a moisture-wicking performance fabric — perfect for casual and athletic footwear where regular socks cause overheating. For toenail fungus patients, keeping the foot environment dry is one of the most impactful interventions. FLAT SOCKS eliminate sock-caused moisture trapping while still protecting the shoe interior from sweat.
Moisture-wicking no-sock inserts supports the practice
Shop at michiganfootdoctors.com/shop/
Not Ideal For: Patients with active open wounds, severe tinea pedis, or anyone who needs full sock coverage for cushioning. Also not a substitute for antifungal treatment.
PowerStep Pinnacle Insoles
Proper arch support with PowerStep Pinnacle insoles helps normalize pressure distribution across the foot — reducing the toe-box crowding that creates the warm, moist microenvironment where fungi thrive. Patients with flat feet or overpronation often have toes that press together, trapping moisture between them. Correcting foot mechanics reduces this risk factor.
Full-length arch support insole — replaces generic insoles
Shop at michiganfootdoctors.com/shop/
Not Ideal For: Patients with high arches requiring neutral or minimal support, or narrow dress shoes where a full-length insole doesn’t fit.
In-Office Treatment at Balance Foot & Ankle
For nail fungus that hasn’t responded to home treatment after 3–6 months, our podiatrists offer prescription nail lacquers (ciclopirox), oral terbinafine therapy with monitoring, professional nail debridement to improve topical penetration, and laser antifungal treatment for appropriate candidates. We also confirm the diagnosis — many nail conditions mimic fungus including nail psoriasis, trauma-related discoloration, and nail melanoma.
Get Your Toenail Fungus Properly Diagnosed
Same-day appointments available. We confirm the diagnosis and prescribe the right treatment.
Book an AppointmentHowell: (810) 206-1402 | Bloomfield Hills: (810) 206-1402
Frequently Asked Questions
How long does it take for home remedies to work on toenail fungus?
You won’t see dramatic results for 3–4 months because the infected nail must physically grow out while new healthy nail grows in from the root. Great toenails grow about 1mm per month — a full new nail takes 12–18 months. That said, you should notice the nail looking less opaque and slightly improved in color within 6–8 weeks if treatment is working. If you see zero change at 3 months, the concentration or remedy type may not be effective against your particular fungal strain.
Can toenail fungus go away on its own without treatment?
Rarely, and it almost never does in adults. Without treatment, dermatophyte infections in the nail plate are generally persistent and slowly progressive — spreading from one nail to adjacent nails and potentially to the skin (tinea pedis). Spontaneous resolution is sometimes seen in superficial white onychomycosis in immunocompetent individuals, but distal subungual onychomycosis (the most common type) virtually never resolves without intervention. Treatment slows the spread and prevents skin complications.
Is toenail fungus contagious?
Yes. Toenail fungus is caused by dermatophytes that spread through direct contact with infected surfaces or through contact with an infected person’s skin and nails. The highest-risk transmission environments are shared showers, pool decks, locker rooms, and nail salons with inadequate sterilization. You can also spread it from one of your own toenails to others. Household members sharing bathroom floors or bathmats are at moderate risk of cross-infection.
Can I paint my toenails if I have fungus?
We recommend against it. Nail polish traps moisture under the nail, creates a barrier that prevents topical antifungal penetration, and makes it harder to monitor treatment progress. If you must paint your nails for a social event, keep it brief and remove the polish as soon as possible. Regular use of nail polish during active fungal treatment significantly slows resolution and may allow the infection to worsen despite treatment.
When should I see a podiatrist for toenail fungus?
See a podiatrist if you have diabetes or circulation problems (any foot nail issue), if you’re unsure whether it’s fungus or another condition (psoriasis, trauma, melanoma), if the infection is spreading, if you have pain or thickening that affects how you walk, or if home and OTC treatments haven’t worked after 6 months. Podiatrists can confirm diagnosis, debride infected nail tissue, and prescribe oral antifungals that are far more effective than any topical.
Sources
- Nenoff P, et al. “Onychomycosis — an update. Part 1: Prevalence, epidemiology, predisposing conditions, and differential diagnosis.” JDDG 2014.
- Syed TA, et al. “Treatment of toenail onychomycosis with 2% butenafine and 5% Melaleuca alternifolia (tea tree) oil in cream.” Tropical Medicine & International Health 1999.
- Derby R, et al. “Novel treatment of onychomycosis using over-the-counter mentholated ointment (Vicks VapoRub).” Journal of the American Board of Family Medicine 2011.
- Nenoff P, et al. “Antifungal activity of the essential oil of Melaleuca alternifolia (tea tree oil) against pathogenic fungi in vitro.” Skin Pharmacol 1996.
- Lipner SR, Scher RK. “Onychomycosis: Treatment and prevention of recurrence.” Journal of the American Academy of Dermatology 2019;80(4):853–867.
Frequently Asked Questions
Can toenail fungus go away on its own?
Almost never. Once a fungal infection establishes in the nail matrix, it rarely self-resolves. The nail acts as a physical barrier protecting the fungus from both topical treatments and the immune system. OTC treatments like Vicks VapoRub and tea tree oil show limited evidence for mild cases, but clinical cure rates are under 20%. Prescription treatment — topical ciclopirox, oral terbinafine, or laser therapy — is typically required for meaningful improvement.
What’s the most effective treatment for toenail fungus?
Oral terbinafine (Lamisil) remains the gold standard with 70–80% clinical cure rates over 12 weeks. Topical treatments (efinaconazole, tavaborole) cure 18–55% but avoid the systemic drug exposure. Laser therapy in our office shows 60–75% improvement rates and is a good option for patients who can’t tolerate oral medication. Combination therapy — laser plus topical — produces better outcomes than either alone. Cure is defined as a fully clear nail, which takes 9–12 months even after the infection is eliminated.
Can toenail fungus spread to other nails or to family members?
Yes to both. Toenail fungus spreads readily via shared surfaces — floors, bath mats, showers, socks. Within the same foot, it typically spreads from nail to nail if left untreated. Family transmission is common in shared showers and from shared nail tools. During treatment, disinfect shower floors weekly, avoid sharing towels or nail clippers, wear flip-flops in shared shower areas, and wash socks in hot water. Treating the shoes is also important — antifungal spray applied inside shoes during treatment prevents reinfection.
Why isn’t my over-the-counter toenail fungus treatment working?
Three common reasons: (1) The infection is in the nail matrix, too deep for topical penetration. (2) The nail is too thick for medication to reach the fungus. (3) What looks like fungus may be nail psoriasis, nail trauma, or a secondary bacterial infection — which don’t respond to antifungals. A nail sample for culture confirms the diagnosis and identifies the specific fungal species, which guides treatment selection. We see patients weekly who’ve spent hundreds of dollars on OTC products without a confirmed diagnosis.
Is toenail fungus dangerous?
In healthy individuals, toenail fungus is primarily a cosmetic and quality-of-life issue. In diabetic patients, patients with peripheral vascular disease, or immunocompromised individuals, it’s a genuine safety risk — the thickened nail causes pressure sores, the infected nail provides an entry point for bacterial infection, and tinea pedis (foot fungus) associated with nail fungus can cause skin breakdown. For these patients, aggressive treatment is medically indicated, not optional.
How long does treatment take?
This is the most important thing to understand about toenail fungus: even after successful treatment kills the fungus, the nail takes 9–12 months to grow out completely. Oral terbinafine is taken for 12 weeks; the fungus is eliminated within that period, but patients expect to see a clear nail immediately and feel the treatment failed. Improvement at 3 months looks like a clear nail growing from the base. Full cosmetic clearance at 12 months. Patience with the process is essential.
Can toenail fungus cause other health problems?
In high-risk patients — yes. The most important association is athlete’s foot (tinea pedis), which frequently co-occurs with nail fungus and can cause skin fissuring that allows bacterial entry. For diabetic patients especially, treating foot fungus is part of diabetic foot care. Severe nail deformity from long-standing fungus can also cause subungual pressure sores, ingrown nails, and difficulty fitting footwear. What starts cosmetic can become functional.
Does insurance cover toenail fungus treatment?
Oral terbinafine is inexpensive and usually covered by insurance with a copay under $30 for a full course. Prescription topical treatments (efinaconazole) are often not covered and cost $400–600 out of pocket. Laser therapy is not covered by insurance but typically costs $400–700 per course of 3 treatments in our office. We’ll discuss what’s appropriate for your case and what your out-of-pocket costs will be before prescribing. Call (810) 206-1402 to check your specific coverage.
What’s the difference between toenail fungus and nail psoriasis?
Both cause nail thickening, discoloration, and deformity — they can look identical to the naked eye. Key differences: psoriasis often causes ‘pitting’ (small dimples in the nail surface), oil-drop spots, and is associated with skin psoriasis elsewhere on the body. Fungus causes more uniform thickening and yellowing. The only definitive differentiation is a nail sample sent for PAS staining and fungal culture. Misdiagnosis is extremely common — we’ve seen patients treat ‘fungus’ for years when they actually had nail psoriasis.
How do I prevent toenail fungus from coming back?
The three most evidence-supported prevention strategies: (1) Antifungal spray or powder in shoes daily — the shoe environment harbors fungal spores even after treatment. (2) Replace old shoes after completing treatment; they may be recontaminating you. (3) Flip-flops in all shared showers, pools, locker rooms. Beyond that: keep nails trimmed short, dry feet thoroughly after bathing (especially between toes), and wear moisture-wicking socks. Recurrence rates are 25–30% at 1 year even with good hygiene.
Same-Week Appointments in Howell & Bloomfield Hills
Three board-certified podiatric surgeons. 1,123+ five-star reviews. Most insurance accepted.
American Academy of Dermatology: Nail Fungus
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.