
Quick answer: White patches or spots on the toenails are most often leukonychia — minor trauma to the nail or keratin granulations from polish — and are usually harmless. Chalky, spreading, or crumbly white areas can signal a fungal infection; if the patches grow or the nail thickens, see a podiatrist to confirm the cause.
Or call: (810) 206-1402
Medically reviewed by Dr. Tom Biernacki, DPM
Board-certified podiatric surgeon | Balance Foot & Ankle
Last reviewed: May 2026
White toenail patches have two entirely different causes — and applying the treatment for one permanently worsens the other. Our podiatrists identify which is which using a single clinical observation that takes under 30 seconds and requires no lab testing. Call (810) 206-1402 — expert podiatric care across Michigan.
White patches, spots, streaks, and bands on toenails are one of the most common nail complaints we evaluate in our Howell and Bloomfield Hills podiatric offices. Most are completely benign — the tiny white spots you’ve had since childhood that grow out and disappear, or the chalky patches left by your last gel manicure. But some white nail changes are the first visible sign of a systemic medical condition or an active fungal infection, and knowing which type you’re looking at changes everything about the appropriate response.
White Patches on Toenails: The 6 Causes at a Glance
White patches on toenails have 6 distinct causes — and the correct treatment depends entirely on which type you have. Keratin granulation (from nail polish acetone) resolves with a 4–6 week polish break and cuticle oil. Fungal white patches (white superficial onychomycosis) require antifungal treatment — oral terbinafine or laser. Leukonychia from minor trauma grows out on its own in 6–12 months. If you are not sure which type you have, a KOH test at our office provides a definitive answer in minutes. (810) 206-1402 — Howell & Bloomfield Hills, MI.
The Most Common Mistake With White Patches on Toenails
The biggest mistake patients make is applying antifungal cream to keratin granulation — treating a non-fungal problem as fungus. This wastes weeks and delays the actual fix (a polish break). The reverse mistake also happens: assuming white patches are just “cosmetic” when they are actually early-stage toenail fungus that will worsen without treatment. The fix: a KOH scraping test takes 2 minutes and definitively tells you which you have. When in doubt, get tested before treating.
Understanding Nail Anatomy: Plate vs. Bed
The critical first step in evaluating white nail changes is understanding where the whiteness originates — because nail plate whiteness and nail bed whiteness have entirely different causes and implications.
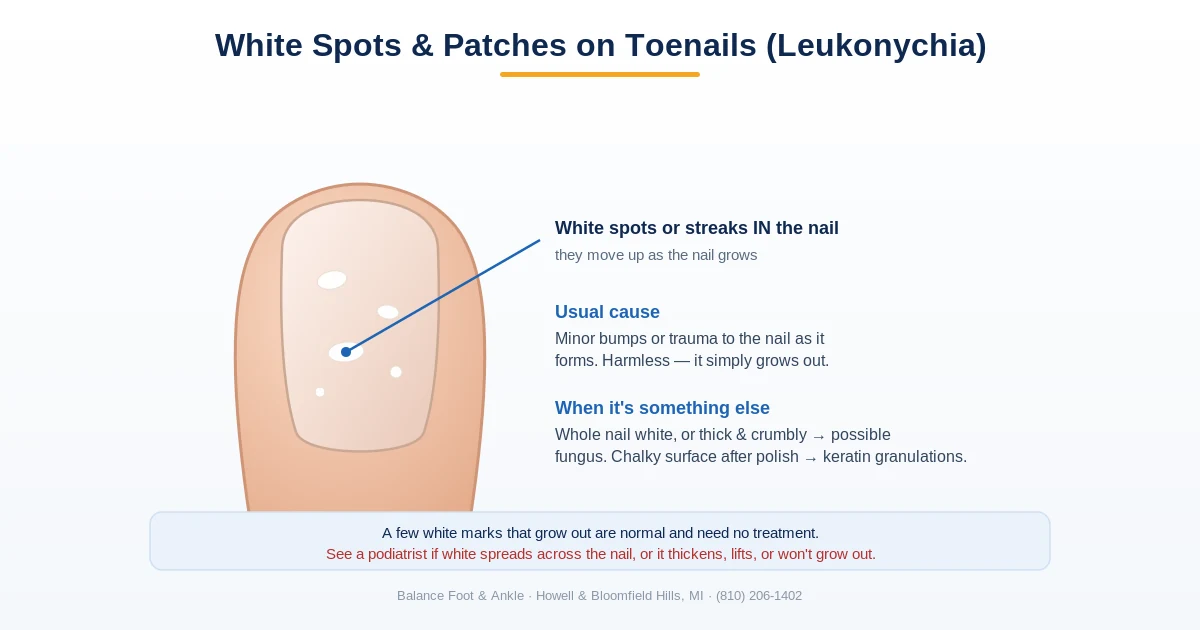
The nail plate is the hard keratinized structure you see and feel — the actual “nail.” It is produced by the nail matrix (the tissue under the skin at the base of the nail). White changes within the nail plate are called true leukonychia — the nail plate itself contains white areas that travel forward as the nail grows.
The nail bed is the pink tissue under the nail plate. Its pink color shows through the translucent nail plate and gives your nail its normal pink appearance. White changes at the nail bed level are called apparent leukonychia — the nail plate is actually translucent and normal, but the bed beneath it appears white, obscuring the normal pink. Apparent leukonychia disappears or changes when you compress the nail (compressing the blood vessels in the nail bed changes the appearance).
Key takeaway: The key diagnostic question for any white toenail change: is the whiteness in the nail plate itself (stays white when you press on the nail) or is it coming from the nail bed beneath (disappears or changes when you compress the nail)? Nail plate whiteness = usually benign trauma or fungal. Nail bed whiteness = potentially systemic disease signal requiring medical evaluation.
Cause 1: True Leukonychia — Trauma Spots (Most Common)
True leukonychia punctata — the small white spots most people have noticed on their nails at some point — is caused by minor, often unnoticed trauma to the nail matrix. Pressing the fingers tightly, a small impact, pedicure tools pressing on the nail base, or even picking at the cuticle can disrupt the nail matrix cells briefly, causing a small area of incompletely keratinized nail cells. These appear white and travel forward with nail growth.
True leukonychia spots are located within the nail plate (they don’t change with nail compression), are typically 1–3mm in size, and grow slowly forward toward the free edge at the rate of nail growth (about 1.5–2mm per month for toenails). They eventually grow to the tip and are trimmed away. No treatment is needed. This is the white nail change that old wives’ tales attribute to calcium or zinc deficiency — those attributions are not supported by evidence. The cause is almost always minor trauma.
Cause 2: Keratin Granulations — After Nail Polish
Keratin granulations are superficial white patches on the nail surface that appear after nail polish removal, particularly after gel or acrylic nails, or after repeated application of dark polishes. The combination of nail polish adhesion and acetone stripping damages the superficial layers of the nail plate — the tightly bonded keratin fibers are disrupted, creating a rough, chalky-white, powdery surface texture.
Keratin granulations are the single most common reason patients present to our office thinking they have toenail fungus. The distribution (immediately visible after nail polish removal), the chalky powdery texture, the lack of nail thickening, and the negative KOH preparation (no fungal hyphae) confirm the diagnosis. Treatment: stop applying nail polish, apply a hydrating nail conditioner or buffered nail hardener, and allow 2–4 months for the affected nail to grow out.
Key takeaway: Keratin granulations — the chalky white patches left on nails after removing dark or gel nail polish — are not a fungal infection. They are surface damage to the nail keratin from the stripping effect of acetone and polish adhesives. They grow out completely over 2–4 months and require no antifungal treatment, despite looking similar to white superficial onychomycosis.
Cause 3: White Superficial Onychomycosis (WSO)
White superficial onychomycosis (WSO) is a fungal infection that invades the surface of the nail plate directly from the top, rather than from the free nail edge or nail bed as in the more common distal lateral subungual onychomycosis (DLSO). The causative organisms include Trichophyton mentagrophytes (most common in WSO), T. rubrum, and occasionally non-dermatophyte molds.
WSO appears as dull, white, opaque patches on the dorsal (top) surface of the nail plate — similar in distribution to keratin granulations but with important distinctions: the white surface is somewhat crumbly or chalky-powdery on scraping but the area beneath feels soft and slightly irregular (versus the smoother base of keratin granulations). A KOH preparation of the scraped material shows branching fungal hyphae, confirming the diagnosis.
WSO is relatively straightforward to treat because the fungus is superficial — mechanical debridement of the white surface combined with topical antifungal agents (ciclopirox nail lacquer, efinaconazole, or amorolfine) penetrates adequately to the infection site. The nail does not need to be penetrated from below. Oral antifungals are reserved for extensive or recurrent WSO or when WSO is accompanied by other nail unit infection.
Key takeaway: White superficial onychomycosis (WSO) is distinguished from keratin granulations by the scraping test: WSO scrapes off easily with a clean blade, exposing a rough, friable nail surface underneath. Keratin granulations also scrape off but leave a smoother nail surface. Both confirm under KOH preparation — dermatophyte hyphae are present in WSO, absent in keratin granulations.
Cause 4: Apparent Leukonychia — Terry’s Nails
Terry’s nails present as nails that are mostly white (occupying 80–100% of the nail), with a narrow 1–2mm band of normal pink or brownish color at the distal free edge. The whiteness reflects the underlying nail bed — the distal nail bed becomes white/pale while the very tip retains its pink capillary blush. This is an apparent leukonychia — pressing on the nail blanches the distal pink band and makes the change more pronounced.
Terry’s nails are associated with systemic conditions: hepatic cirrhosis (most classically), congestive heart failure, type 2 diabetes, and chronic kidney disease. They reflect changes in the nail bed microcirculation and connective tissue. While they can occasionally occur as a normal aging variant in older adults, new-onset Terry’s nails warrant evaluation for the associated systemic conditions.
Cause 5: Muehrcke’s Lines
Muehrcke’s lines are pairs of parallel white transverse bands running across the nail, separated by areas of normal nail. They are apparent leukonychia — located in the nail bed, not the plate — and disappear with pressure. Unlike true leukonychia bands (Mees’ lines), they do not move with nail growth because they reflect a persistent change in the nail bed.
Muehrcke’s lines are associated with hypoalbuminemia — low blood albumin levels. The differential diagnosis of hypoalbuminemia includes nephrotic syndrome, hepatic disease, malnutrition, and protein-losing enteropathy. The lines typically disappear after albumin levels are normalized. Their presence alongside systemic symptoms — edema, fatigue, abdominal swelling — warrants prompt medical evaluation.
Cause 6: Proximal Subungual White Onychomycosis
Proximal subungual onychomycosis (PSO) is a rare pattern of onychomycosis where the fungus invades from the proximal nail fold (the skin at the base of the nail) rather than the free edge. It presents as a white or opaque area at the base (proximal end) of the nail that gradually moves forward. In immunocompetent patients, PSO is uncommon. Its presence is considered a marker for HIV infection and significant immunosuppression — the nail fold skin’s immune barrier normally prevents this invasion route. Any patient with PSO who has not been tested for HIV should be evaluated.
⚠️ White nail changes that warrant medical evaluation
- White nails affecting most of the nail (Terry’s nails — white with a narrow pink or brown band at the tip) — associated with liver disease, heart failure, diabetes, kidney disease
- Parallel white bands across the nails (Muehrcke’s lines) — associated with hypoalbuminemia from nephrotic syndrome, liver disease, or malnutrition
- White spots in the lower (proximal) nail — proximal subungual white onychomycosis is associated with HIV immunosuppression
- Systemic symptoms (fatigue, weight loss, jaundice, swelling) alongside nail changes — the nails may be signaling an internal disease process
- White patches that are not growing out over months and are spreading to more nails — needs nail KOH and culture
White Toenail Patches: The 6 Causes at a Glance
| Cause | What you see | Plate or nail bed? | What it signals |
|---|---|---|---|
| True leukonychia (trauma spots) | Small white spots or dots | Nail plate — grows out | Harmless; the most common cause |
| Keratin granulations (after polish) | Chalky white surface patches after polish removal | Plate surface | Cosmetic, not fungus; clears in weeks |
| White superficial onychomycosis (WSO) | White, crumbly patches on the nail surface | Plate surface (fungal) | A treatable fungal infection |
| Apparent leukonychia (Terry’s nails) | Nail ~80–100% white with a thin normal band at the tip | Nail bed — doesn’t grow out | Can reflect systemic disease — worth evaluating |
| Muehrcke’s lines | Paired white bands that fade when you press the nail | Nail bed | Linked to low blood protein / systemic illness — worth evaluating |
| Proximal subungual onychomycosis (PSO) | White starting at the base of the nail | Plate, from the base (fungal) | Rare; can signal a weakened immune system |
How We Diagnose White Nail Changes
In our clinic, evaluation of white nail patches follows a systematic approach: nail plate vs. nail bed location (pressure test), distribution pattern (single spot vs. bands vs. whole nail), relationship to nail polish history or trauma, KOH preparation of nail scrapings (definitive for fungal vs. non-fungal), and nail culture if atypical organisms are suspected. When systemic conditions are on the differential, we coordinate with primary care for albumin, liver function, and metabolic panels.
For the full picture — causes, diagnosis, and all treatment options — see our complete toenail fungus guide.
Frequently Asked Questions
What deficiency causes white spots on toenails? The common belief that white spots indicate calcium or zinc deficiency is not supported by clinical evidence. Studies comparing serum mineral levels between patients with and without nail leukonychia have found no consistent difference. The spots are almost always caused by minor nail matrix trauma. True nutritional deficiency nail changes (koilonychia from iron deficiency, Muehrcke’s lines from hypoalbuminemia) have distinctive patterns different from the typical small white spot.
How do I tell if my white nail patches are fungal? KOH preparation is the definitive test — a nail scraping examined under microscopy. Clinically, fungal WSO tends to produce dull, chalky patches with a slightly soft crumbly texture on scraping, and may be associated with nail thickening in more advanced cases. Keratin granulations are surface-only, appear immediately after nail polish removal, and the nail plate itself is normal in thickness and hardness. When in doubt, a podiatric evaluation resolves the question in one visit.
Do white spots on toenails go away on their own? True leukonychia spots from trauma grow out naturally — they cannot disappear before they reach the free edge and are trimmed. This takes months for toenails (slow nail growth). Keratin granulations grow out over 2–4 months with a nail polish break. WSO does not resolve without antifungal treatment and will spread over time. Apparent leukonychia (Terry’s nails, Muehrcke’s lines) resolves when the underlying systemic condition is treated.
What causes white patches on toenails?
White patches on toenails (leukonychia) have several causes: superficial white onychomycosis (fungal), minor trauma creating air pockets under the nail plate, psoriasis, and systemic conditions. Fungal white patches sit on the nail surface and scrape off easily; traumatic white spots do not.
Are white spots on toenails always fungus?
No. The most common cause of white spots in children and young adults is minor trauma (leukonychia punctata). Fungal white patches appear on the nail surface and can be scraped off with a blade. A podiatrist can confirm with a nail clipping and KOH test.
How do you treat white patches on toenails?
Treatment depends on the cause. Superficial white onychomycosis responds to topical antifungals such as ciclopirox or efinaconazole. Traumatic white spots resolve as the nail grows out. Nail psoriasis requires dermatologic management. See a podiatrist if patches spread or the nail thickens.
The Bottom Line
White patches on toenails are most often benign — minor trauma spots or the aftermath of nail polish. Keratin granulations are the most common cause of clinic visits, and the treatment is simple: polish break. The important cases to identify are WSO (needs antifungal), Terry’s nails and Muehrcke’s lines (need systemic evaluation), and proximal subungual pattern in a young or ill patient (HIV screening). The nail plate-vs-nail-bed distinction and a simple KOH scraping resolve the vast majority of diagnostic questions in a single visit.
American Academy of Dermatology: Nail Fungus
Sources
- Baran R, Dawber RPR, de Berker DAR, et al. Baran and Dawber’s Diseases of the Nails and Their Management. 4th ed. Wiley-Blackwell; 2012.
- Fawcett RS, Linford S, Stulberg DL. Nail abnormalities: clues to systemic disease. Am Fam Physician. 2004;69(6):1417-1424.
- Gupta AK, Sibbald RG, Lynde CW, et al. Onychomycosis in children: prevalence and treatment strategies. J Am Acad Dermatol. 1997;36(3 Pt 1):395-402.
- Lipner SR, Scher RK. Onychomycosis: treatment and prevention of recurrence. J Am Acad Dermatol. 2019;80(4):853-867.
- Piraccini BM, Alessandrini A. Onychomycosis: a review. J Fungi (Basel). 2015;1(1):30-43.
Ready to Get Relief?
Same-day appointments available in Howell & Bloomfield Hills, MI
4.9★ | 1,123 Reviews | 3,000+ Surgeries
For a complete guide to toenail conditions and treatment, see our Toenail Fungus & Nail Condition Treatment Guide.
If white patches appeared after nail polish use, the cause may be keratin granulations — explained in detail in our guide to White Chalky Toenails from Nail Polish.
📋 Dr. Tom Biernacki, DPM, FACFAS answers:
White patches on toenails have 6 main causes that look different under a podiatrist’s scope: (1) keratin granulations from nail polish — chalky white, surface only; (2) superficial white onychomycosis (fungal) — powdery, scrapes off; (3) true leukonychia — white spots from minor nail matrix trauma; (4) proximal subungual onychomycosis — starts at base, immune compromise; (5) distal onychomycosis — yellow-white with thickening; (6) nail psoriasis — pitting plus white patches. Surface pattern matters: if it scrapes off with a file, it’s usually keratin granulation or superficial fungus. If it’s under the nail, treat as onychomycosis.
For a complete guide to all toenail fungus types, causes, and treatment options, visit our Toenail Fungus Treatment Guide. If you have heard about Vicks VapoRub as a remedy, read our podiatrist’s honest assessment: Does Vicks Really Work for Toenail Fungus?
Related white-nail guides
Sorting out white patches on the nails? Compare these:
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.