
Ready to be seen? Book a real appointment time online, 24/7 — Howell or Bloomfield Township. Same-week openings are usually available.
Where Exactly Is the Bump? That One Question Narrows It Down Fast
Almost everyone who searches for a bone sticking out on the outside of the foot is describing one of about five things, and the fastest way to tell them apart is not what the bump looks like but where along the foot it sits. Run a finger down the outer edge of your foot from the little toe back towards the heel and note where the prominence is.
- Roughly halfway along the outer edge, level with the middle of your arch. This is by far the most common location, and it is almost always the base of the fifth metatarsal. Usually normal anatomy. Sometimes a fracture.
- Near the front, just behind the little toe. That is a different bone entirely and points towards a tailor’s bunion, also called a bunionette.
- At the back, on or above the heel bone. That is Haglund’s deformity territory rather than a lateral midfoot bump, and it behaves differently.
- Soft, squishy and movable rather than hard. If it does not feel like bone, it very often is not — a ganglion cyst is the usual explanation.
- A bump that is new, on a foot with reduced sensation, and the foot is warm and swollen. Stop reading and call someone today. This one is covered at the bottom of this page and it is the reason we wrote it.
The Usual Answer: The Base of Your Fifth Metatarsal
The fifth metatarsal is the long bone leading to your little toe, and at its back end it flares into a knob called the styloid process. In a lot of perfectly normal feet that knob is prominent enough to see and feel, and people notice it in their thirties or forties and assume something has changed. Two useful checks: look at the other foot, because normal anatomy is usually symmetrical, and ask yourself honestly whether it is genuinely new or whether you simply started paying attention to it.
A prominent styloid becomes a problem rather than a feature for fairly mechanical reasons. People who walk on the outside of the foot, which is called supination, load that edge harder than average. Higher-arched feet sit more on the lateral column. Narrow or stiff shoes press directly on the knob. What hurts in those cases is generally not the bone itself but the tissue caught between the bone and the shoe: a bursa, the peroneal tendons that run right past it, or a callus that has built up over the prominence. That distinction matters because it means the treatment is usually about offloading and footwear rather than about the bump.
A Bump That Appeared Suddenly or After a Twist Is a Different Story
If the prominence showed up after rolling your ankle, stepping off a kerb or landing awkwardly, the working assumption should be a fracture until an X-ray says otherwise. This is one of the most frequently missed injuries in the foot, because the mechanism is identical to a routine ankle sprain and the swelling is in roughly the same neighbourhood.
The clinical distinction is simple to apply. A lateral ankle sprain is tender below and in front of the ankle bone, over the ligaments. A fifth metatarsal base fracture is tender on the bone itself, a couple of inches further forward, at the middle of the outer edge of the foot. If you press there and it is sharply, specifically painful, that needs imaging — not another week of ice and elevation. If that is the spot you are pressing, you can book an evaluation online now in Howell or Bloomfield Township.
Avulsion fracture versus Jones fracture: not interchangeable
Two fractures happen within about an inch of each other here, and they behave completely differently.
An avulsion fracture pulls a fragment off the very tip of the styloid, where the peroneus brevis tendon and part of the plantar fascia attach. It is the more common of the two, it has a good blood supply, and it generally heals well with a stiff-soled shoe or boot and sensible activity limits.
A Jones fracture sits slightly further forward, at the junction where the flared base narrows into the shaft. That precise zone has a notoriously poor blood supply, and as a result Jones fractures have a genuine tendency to heal slowly, to fail to heal at all, or to re-break later. They are treated far more seriously: often a period of not putting weight on the foot, and in active people or athletes, surgical fixation with a screw is frequently recommended as the primary treatment rather than as a rescue. Being told you have “a little fracture in the side of the foot” is not enough information — which of these two it is changes the whole plan.
Tailor’s Bunion: The Bump Nearer the Little Toe
If the prominence is at the front of the outer edge, right behind the little toe rather than back at the arch, it is a bunionette. The name is apt: it is the same process as a bunion but at the opposite side of the foot, with the fifth metatarsal drifting outward and the little toe angling inward. It got the name tailor’s bunion from tailors who sat cross-legged with the outer edge of the foot pressed against the floor all day.
Unlike a prominent styloid, a bunionette is usually progressive, so people describe it as slowly worsening over years rather than as a bump that has always been there. The symptoms come from friction: a hard callus over the bump, redness, an inflamed bursa, and shoes that fit everywhere except across that one point. Wider footwear, padding and offloading handle most cases well. Surgery exists and works, but it is for people whose symptoms persist despite genuinely appropriate shoes, not a first step. One weight-bearing x-ray settles the accessory-bone-versus-fracture question in a single visit, and it changes how the next six weeks go. Book an x-ray visit online.
A Growing Child With a Painful Bump There: Iselin’s Disease
If the person with the prominent, tender bone on the outside of the foot is between about eight and fourteen, the answer is usually different from the adult one — and it is one of the more commonly missed diagnoses in a young athlete’s foot.
The base of the fifth metatarsal has its own growth plate, and it sits at an angle to the shaft rather than across it. The peroneus brevis tendon pulls directly on that growth plate with every push-off and every sideways cut. In an active child — soccer, basketball, dance, gymnastics — that repeated traction irritates the growth plate. The result is Iselin’s disease: a tender, sometimes visibly enlarged prominence on the outer border of the foot that hurts with activity and settles with rest.
Two things make it worth knowing about:
- On X-ray, the open growth plate can be mistaken for a fracture line. It runs obliquely, it is symmetrical with the other foot, and it is normal anatomy. Comparing both feet usually settles it in seconds — a genuine avulsion fracture runs across the bone, not along it.
- It is self-limiting but not self-managing. It resolves as the growth plate closes, but a child who keeps playing through it stays sore for months. Relative rest, activity modification, a stiffer-soled shoe, calf and peroneal stretching, and occasionally a short period in a boot for a bad flare will shorten the whole episode considerably.
A child with pain over the outer midfoot that has lasted more than two or three weeks deserves an examination rather than more rest — partly to confirm Iselin’s, and partly because a stress fracture at that same site is far less forgiving.
Accessory Bones: When the Extra Bone Was Always There
Roughly one person in ten has an extra small bone somewhere in the foot that most people do not. These are normal anatomical variants, present from birth, and they are usually silent for decades — until footwear, a change in activity, or an injury makes one of them announce itself. Two of them sit in exactly the area this page is about.
Os peroneum
A small bone embedded within the peroneus longus tendon as it curves under the cuboid, on the outer border of the foot just behind the fifth metatarsal base. It is present in a substantial minority of feet and is normally symptomless.
It matters when it becomes painful — painful os peroneum syndrome. That can follow a direct blow, an inversion sprain, or a tear of the tendon around it, and it produces pain and tenderness slightly behind and below the fifth metatarsal base, worse when you push the foot outward against resistance. On X-ray, an os peroneum that has fractured or separated will look displaced compared with the other foot, which is why comparison views matter here too.
Os vesalianum
A rarer accessory bone sitting immediately at the tip of the fifth metatarsal base, inside the peroneus brevis tendon. Its main clinical significance is that it is routinely mistaken for an avulsion fracture on X-ray by anyone not looking for it. The distinguishing features: smooth, rounded, corticated edges rather than the sharp irregular margin of a fresh break — and, again, the same appearance on the opposite foot.
Being told you have a fracture that is actually an accessory bone leads to weeks of unnecessary immobilisation. Being told an actual fracture is an accessory bone leads to a non-union. It is worth getting right.
A cuboid prominence
Slightly further back along the outer border, the cuboid itself can feel prominent, particularly in a high-arched foot where the outer column carries more load than it should. This is usually normal bone in an unusual alignment rather than a growth, and it responds to offloading the lateral column with an orthotic rather than to anything surgical.
If the Bump Is on the Inside of the Foot Instead
People search for “a bone sticking out on the side of my foot” from both sides, so it is worth naming the inner-border equivalent briefly.
A prominent bone on the inside of the arch, roughly level with and just below the inner ankle bone, is most often an accessory navicular — an extra bone at the point where the posterior tibial tendon attaches. Like the accessory bones above it is a normal variant, present in perhaps one foot in ten, and often silent until adolescence or until a sprain irritates it.
It matters more than most accessory bones because the posterior tibial tendon is the main dynamic support of the arch. When the attachment is disrupted, arch support can be compromised, and an accessory navicular is a recognised contributor to a painful flatfoot in a teenager. Treatment starts with an orthotic that supports the arch and takes tension off the tendon; surgery to remove the fragment and reattach the tendon is reserved for cases that do not settle.
If you have a bony prominence on either border of your foot that has become painful, changed, or started catching in shoes, it can be identified quickly with an examination and a weight-bearing X-ray — ideally with comparison views of the other foot. Balance Foot & Ankle sees patients in Howell (4330 E Grand River Ave, Howell, MI 48843) and Bloomfield Township (43494 Woodward Ave #208, Bloomfield Township, MI 48302). Call (810) 206-1402.
If It Is Soft and Moves, It Is Probably Not Bone
A ganglion cyst is a fluid-filled sac arising from a joint capsule or tendon sheath, and it turns up on the outside of the foot often enough to be worth knowing. The giveaways are that it feels firm and rubbery rather than rock-hard, it may be slightly movable, and it frequently changes size — larger after a long day, smaller after rest. Old advice to hit them with a heavy book is genuinely a bad idea; they can be aspirated in the office, and the ones that recur can be removed properly.
When a New Bump on the Foot Is a Same-Day Problem
There is one presentation here that is not a nuisance bump, and it is the reason we would rather you read this page than guess. If you have diabetes, peripheral neuropathy or any other cause of reduced sensation in your feet, and a new bony prominence appears on the side or the bottom of the foot, and that foot is warm, swollen and often red, that combination should be assessed immediately. It may be Charcot neuroarthropathy.
In Charcot, the bones and joints of an insensate foot weaken and begin to collapse, frequently without significant pain because the nerves that would normally report it are not working. The affected foot is often noticeably hotter than the other one. It is regularly mistaken for cellulitis, gout, or a sprain, and treated as such for weeks.
The cost of that delay is high, because continuing to walk on a foot in the active phase is what drives the collapse. Caught early and offloaded, the foot can often be preserved in a functional shape. Caught late, the result can be a permanently deformed, rocker-bottomed foot that ulcerates where the new prominence rubs, and those ulcers are how people lose limbs. If this paragraph describes your foot, please do not wait to see whether it settles down on its own.
Quick answer: A protruding bone on the outside of the foot is most often a prominent fifth-metatarsal styloid, a bunionette (tailor’s bunion), or an accessory navicular, and sometimes an old fracture or arthritis. If it is painful, growing, or red, see a podiatrist; many cases respond to wider shoes and padding before any procedure is considered.
Board-certified foot & ankle surgeon · Balance Foot & Ankle, Howell & Bloomfield Hills, MI · Last reviewed: June 2026
Where the protrusion sits on the outside of the foot is more diagnostic than how it feels. A bony prominence at the base of the fifth toe has a different cause, treatment, and timeline than one at the midfoot — even if both hurt in the same way. Of the 5 structural causes Dr. Tom distinguishes in practice, 3 are completely benign and self-limiting, 1 requires a specific shoe accommodation, and 1 needs imaging within 48 hours to rule out a stress fracture. The location pattern that should trigger immediate evaluation is described in the differential section below. Book online or call (810) 206-1402 — same-day X-ray at Howell or Bloomfield Hills.
Most Common Mistake
Assuming every bump on the outside of the foot is the same and treating it with a generic pad. The outer foot harbors 5 distinct conditions: tailor bunion, ganglion cyst, Jones fracture callus, peroneal tendon subluxation, and fifth metatarsal avulsion fracture — each requiring completely different management. A soft movable bump is almost certainly a ganglion cyst; a firm painful bump at the base of the little toe is likely a tailor bunion; sudden onset after ankle inversion warrants fracture imaging before any padding or bracing.
Quick Answer: Protruding Bone on the Outside of the Foot
A bony prominence on the outside of the foot is most often a tailor’s bunion (bunionette) — a gradual outward drift of the 5th metatarsal head that creates a bony bump near the little toe. It is not a fracture and not dangerous, but it causes pain with narrow shoes. The second most common cause is a prominent peroneal tubercle. If the bump appeared suddenly after a fall or roll, get an X-ray the same day to rule out a Jones fracture. Call (810) 206-1402 — Balance Foot & Ankle, Howell & Bloomfield Hills, MI.
The Most Common Mistake With a Protruding Bone on the Outside of the Foot
When a bony bump needs surgery: If a prominent bone on the outside of the foot stays painful despite padding, shoe changes, and orthotics, surgical removal is sometimes the answer. Our board-certified foot & ankle surgeons in Howell and Bloomfield Hills can evaluate whether the prominence should be addressed surgically.
Have a painful bump or protruding bone on your foot?
Board-certified podiatric surgeons treat bunionettes, stress fractures, cysts, and more. Same-week appointments in Howell & Bloomfield Hills, MI. Most insurance accepted.
Book an Appointment → ☎ (810) 206-1402The most common mistake is assuming a bony prominence that appeared after an ankle roll is just a bruise. The base of the 5th metatarsal — exactly where the outer foot bump sits — is one of the most commonly fractured bones in the foot (Jones fracture and avulsion fracture). Both fractures can be walked on, at least briefly, after the injury. The rule: any new bony prominence after a trauma event needs an X-ray. A missed Jones fracture treated as a sprain frequently progresses to a non-union requiring surgery.
Protruding Bone on the Outside of Your Foot: What Is It? (6-Condition Guide)
A protruding bone on the outside of the foot is one of the most common reasons patients present to our podiatry office — and it’s one of the most misunderstood. Most patients assume any bony bump on the lateral foot is a broken bone or something that “appeared overnight.” In reality, six distinct conditions cause this presentation, each with a completely different cause, treatment, and prognosis.
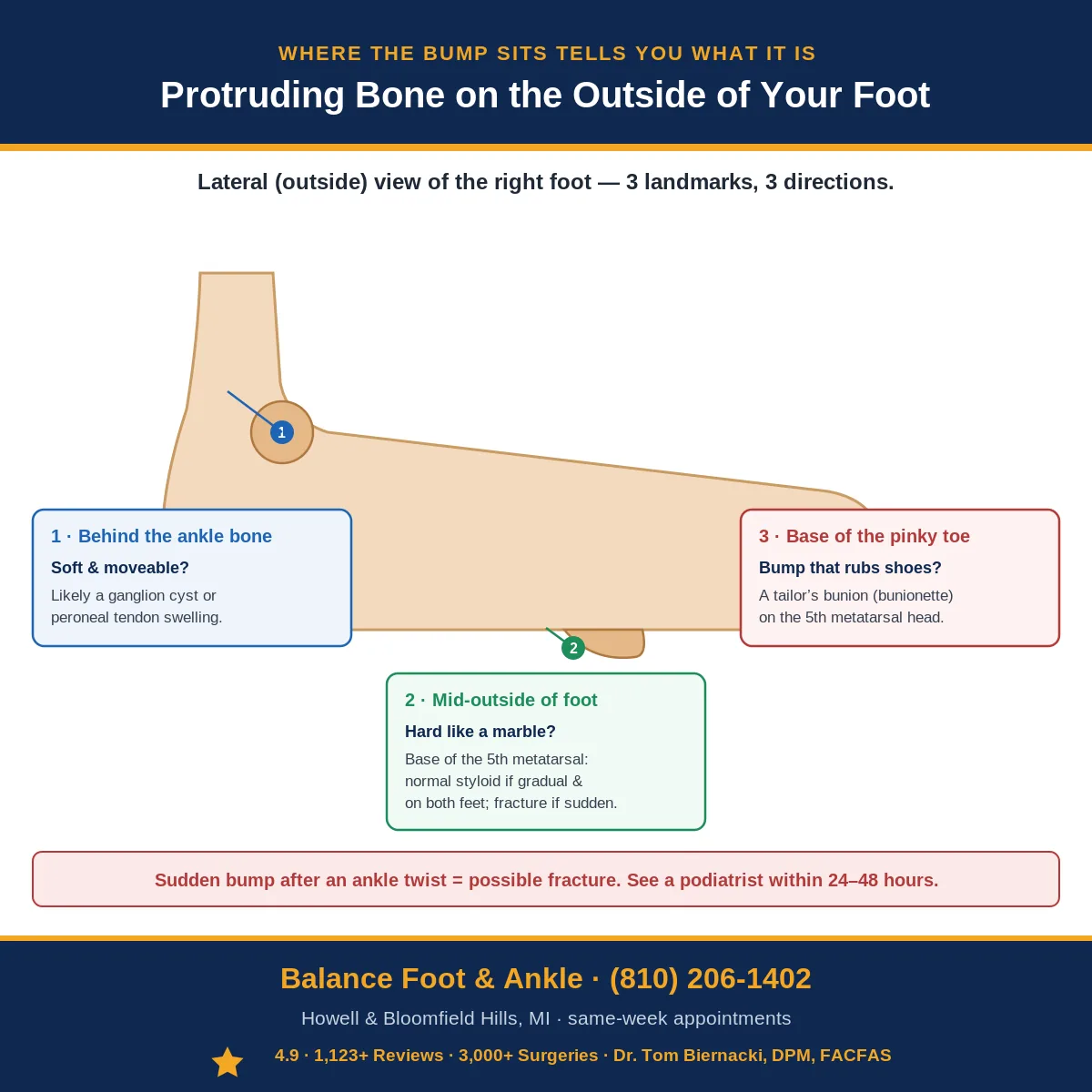
The location of the bump on the outside of your foot narrows the diagnosis dramatically. The lateral foot has three bony landmarks: the base of the 5th metatarsal (mid-lateral foot), the styloid process (the prominent bump at the base of the 5th MT), and the lateral malleolus (the ankle bone). The chart below maps the exact location to the most likely diagnosis.
Protruding Bone Outside of Foot: 6 Conditions by Location
| Condition | Exact Location | Cause | Pain Pattern | Key Diagnostic Sign | Treatment |
|---|---|---|---|---|---|
| 5th Metatarsal Styloid Process (Normal Anatomy) | Mid-lateral foot — bony prominence at base of 5th metatarsal; always present; visible in thin individuals | Normal anatomy — peroneus brevis tendon attaches here; not pathological; becomes apparent with weight loss or foot swelling | None, or mild tenderness only if directly bumped; no activity-related pain | Bilateral (same bump on both feet); no acute onset; X-ray shows normal styloid without fracture | No treatment needed; reassurance; wide-toe-box shoes if rubbing against footwear |
| 5th Metatarsal Avulsion Fracture | Base of 5th metatarsal — identical location to styloid process, but sudden onset with inversion injury | Forced ankle inversion causes peroneus brevis tendon to avulse the styloid tip; one of the most common foot fractures | Sudden severe pain at lateral foot after ankle twist; difficulty weight-bearing; swelling and bruising within hours | Acute onset with injury mechanism; point tenderness at 5th MT base; X-ray confirms avulsion fragment with sharp edges (vs. smooth bipartite styloid) | Most avulsions: hard-soled shoe or CAM boot × 4–6 weeks, weight-bearing as tolerated. Displaced fragments >2mm or instability: surgical fixation |
| Jones Fracture | Proximal 5th metatarsal shaft — just distal (past) the styloid process, at the metaphyseal-diaphyseal junction (zone 2) | Repetitive stress or sudden inversion; watershed blood supply zone — poor healing; higher non-union risk than avulsion fracture | Lateral foot pain at or just distal to the styloid; may have had preceding ache (stress reaction) before acute fracture; insidious or sudden | Tenderness slightly distal to styloid; X-ray shows transverse fracture at metaphyseal-diaphyseal junction; crucial to distinguish from avulsion (different treatment) | Non-weight-bearing CAM boot × 6–8 weeks; surgical fixation (intramedullary screw) often recommended for athletes or high-risk for non-union |
| Tailor’s Bunion (Bunionette) | 5th metatarsal head — at the base of the little toe; distal lateral foot; may have red, irritated skin over bump | Lateral bowing of 5th metatarsal with prominent metatarsal head; narrow shoes compress the 5th MT head against shoe; hereditary bone structure | Gradual, progressive; worse with tight or narrow shoes; bursitis over bump (red, tender, swollen); no acute injury | Bony prominence at 5th MT head with overlying bursa or callus; bilateral in most cases; X-ray shows increased 4th-5th intermetatarsal angle; worse with narrow shoes | Wide toe-box shoes; custom orthotic to offload 5th MT head; bursal injection if inflamed; bunionette correction surgery for severe structural deformity |
| Peroneal Tendon Subluxation or Tenosynovitis | Posterior to lateral malleolus; soft tissue bump rather than hard bone; may be visible tendon when ankle moves | Peroneal retinaculum tear allows tendons to sublux over lateral malleolus; or tenosynovitis (inflammation within tendon sheath) creates soft tissue swelling | Lateral ankle pain + sensation of snapping or popping; pain with ankle eversion; swelling over peroneal tendons (posterior to malleolus, not at base of 5th MT) | Soft, mobile swelling (vs. hard bone); peroneal subluxation test positive (dorsiflexion + eversion causes visible tendon snap); ultrasound confirms | Acute subluxation: CAM boot + surgical retinaculoplasty for active patients; tenosynovitis: PT + brace; chronic: surgical stabilization |
| Ganglion Cyst (Lateral Foot) | Variable — can occur anywhere on lateral foot; often near joints or tendon sheaths; soft, fluctuant (jelly-like), not hard | Herniation of joint capsule or tendon sheath filled with synovial fluid; benign; may enlarge and shrink spontaneously | Usually painless; may cause pressure pain with certain shoes; no trauma history; may appear and disappear | Soft, fluctuant, transilluminates (light passes through when illuminated) — confirms fluid-filled cyst; not fixed to skin; X-ray shows no bone abnormality | Observation (50% resolve spontaneously); aspiration (recurrence rate 50%); surgical excision for persistent symptomatic cysts (lower recurrence) |
How to Tell Which Bony Bump You Have: The 3-Step Self-Assessment
| Step | What to Check | Result → Diagnosis Direction |
|---|---|---|
| Step 1: When Did It Appear? | Did the bump appear suddenly (same day or overnight) after an injury? Or has it been there gradually for months/years? | Sudden after ankle twist → fracture (avulsion or Jones) — see a podiatrist within 24–48 hours. Gradual/always been there → styloid process, tailor’s bunion, or ganglion — less urgent |
| Step 2: Is It Hard Bone or Soft Tissue? | Press firmly on the bump. Is it completely hard like a marble? Or does it have any give (soft, moveable, fluctuant)? | Completely hard = bone (styloid process, fracture, tailor’s bunion). Soft, jelly-like = ganglion cyst. Soft + over the tendon behind ankle = peroneal swelling |
| Step 3: Exactly Where Is It? | At the base of the pinky toe (distal lateral foot)? At the midpoint of the outside of the foot? Or behind the ankle bone? | At pinky toe base → tailor’s bunion. Mid-lateral foot (base of 5th metatarsal) → styloid process, avulsion fracture, or Jones fracture. Behind ankle → peroneal tendon issue |
When Is a Protruding Bone on the Outside of the Foot an Emergency?
| Sign / Symptom | What It Suggests | Action |
|---|---|---|
| Sudden severe pain after ankle twist + unable to weight-bear | Avulsion fracture or Jones fracture — Ottawa Rules indicate X-ray needed | Urgent care or ED within hours; do NOT walk on it; ice and elevate |
| Open wound or skin breakdown over the bump | Fracture with soft tissue involvement OR infected bursa over tailor’s bunion/styloid | Same day podiatrist visit; risk of infection spreading to bone |
| Diabetic patient with new bump or skin redness | Risk of Charcot fracture (neuropathic bone destruction) or infected callus | Urgent podiatrist within 24 hours; Charcot can destroy the foot if untreated |
| Bump growing rapidly (weeks, not years) | Tumor (rare but possible); osteochondroma; sarcoma (extremely rare) | Podiatrist within 1–2 weeks; X-ray and possible MRI to rule out neoplasm |
| Numbness or tingling around the bump | Nerve compression from the bony prominence or adjacent ganglion | Podiatrist within 2–4 weeks; sural nerve compression can worsen without treatment |

You can feel a bone sticking out the side of your foot. It’s been there for a while but suddenly it bothers you. There’s an explanation.
You’re in the right place. Dr. Tom Biernacki, DPM, FACFAS — board-certified foot & ankle surgeon with 3,000+ surgeries — explains exactly what a protruding bone on the outside of the foot means and what works. Book online or call (810) 206-1402 for same-day appointment at Howell or Bloomfield Hills.
What causes a protruding bone on the outside of the foot?
A protruding bone on the outside of the foot is usually an enlarged styloid process of the fifth metatarsal (a bunionette or tailor’s bunion), an accessory navicular, an old healed avulsion fracture, or arthritis at the cuboid-fifth metatarsal joint. X-ray confirms the source. Conservative treatment includes wider shoes, padding, and orthotics; surgery is reserved for chronic pain.
Protruding Bone on Outside of Foot: Diagnosis & Treatment Guide
In This Article
- Protruding Bone on the Outside of Your Foot: What Is It? (6-Condition Guide)
- How to Tell Which Bony Bump You Have: The 3-Step Self-Assessment
- When Is a Protruding Bone on the Outside of the Foot an Emergency?
- What causes a protruding bone on the outside of the foot?
- Comparison Table: Differential Diagnosis of Lateral Foot Bumps
- Frequently Asked Questions About Lateral Foot Bumps
- The Most Common Mistake We See
Frequently Asked Questions
Should I worry about a bone bump on my foot?
Painless slow-developing bumps are usually benign (tailors bunion or accessory bone). Painful or rapidly enlarging bumps need imaging.
Can I shrink a bone bump on the outside of my foot?
No – bony prominences do not shrink. You can reduce friction with shoe modifications and pads. Surgery is reserved for persistent pain.
What is a tailors bunion?
A bony prominence at the base of the fifth (pinky) toe, similar to a bunion of the big toe. Common in narrow shoes.
Dr. Tom Biernacki, DPM explains what causes bumps and lumps on the foot, how to distinguish between a tailor’s bunion, accessory bone, and other bony prominences, and when surgical intervention is warranted.

What Helps: Dr. Tom’s Recommended Products for Lateral Foot Pain
When a tailor’s bunion or protruding bone creates friction and inflammation, the right combination of off-loading and targeted pain relief makes a significant difference before considering any surgical option.
Affiliate disclosure: Balance Foot & Ankle earns a commission from qualifying Foundation Wellness purchases at no extra cost to you.
Doctor Hoy’s Natural Pain Relief Gel — Natural topical pain relief I use in our clinic. Arnica + camphor formula reduces tissue-level inflammation at the fifth metatarsal. Apply 3–4x daily directly to the outer foot. Doctor Hoy’s botanical formula addresses inflammation rather than masking it — important when managing chronic friction pain.
PowerStep Pinnacle Insoles — The OTC orthotic I recommend most in our clinic. Proper arch support off-loads the fifth metatarsal head and distributes pressure evenly across the foot, reducing the friction and inflammation driving your pain. Medical-grade support at a fraction of custom orthotic cost.
Lateral Foot Pain Not Improving?
If the pain is in the soft tissue along the outer edge rather than the bone itself, the cause is often tendon-related — see our guide to peroneal tendonitis treatment, the leading cause of lateral foot and ankle pain.
A protruding bone causing persistent pain after 4–6 weeks of home care may have a structural cause requiring imaging or clinical intervention. Same-day appointments available at both our Howell and Bloomfield Hills locations.
⚠️ When to see a podiatrist for a protruding bone on the outside of your foot:
- Sudden onset after ankle twist or inversion injury — acute avulsion or Jones fracture until proven otherwise; needs same-day X-ray
- Inability to bear weight on the foot — fracture red flag requiring urgent evaluation
- Swelling, bruising, or warmth around the bump — inflammatory or traumatic cause, not a benign bony variant
- Bump that is rapidly enlarging — bone tumor, ganglion, or infection must be ruled out
- Pain that wakes you at night or is present at rest — aggressive pathology requires imaging
- You have diabetes or poor circulation — any new foot deformity in a diabetic foot is urgent; Charcot arthropathy can present as a lateral prominence
- Bump is warm, red, and tender with fever — septic arthritis or osteomyelitis requires emergency evaluation
Call us same-day: (810) 206-1402 — or book online →
📖 Related: Complete Bunion & Tailor’s Bunion Hub: Causes, Treatment & Surgery →
A prominently protruding bone on the outside of the foot is most often the styloid process of the fifth metatarsal. The American Academy of Orthopaedic Surgeons notes this area is particularly prone to avulsion fractures from ankle sprains, underscoring the importance of professional evaluation for any acute bump.
Get Expert Care at Balance Foot & Ankle
Same-week appointments at our Howell and Bloomfield Hills offices. Board-certified podiatric surgeons. Most insurance accepted.
For a complete clinical overview: Heel Pain Causes & Treatment Guide — every cause of foot and heel pain diagnosed
Dr. Tom Biernacki, DPM is a double board-certified podiatrist and foot & ankle surgeon at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has reached over one million views.
- Plantar Fasciitis: Diagnosis and Conservative Management (PubMed)
- Plantar Fasciitis (APMA)
- Diagnosis and Treatment of Plantar Fasciitis (PubMed / AAFP)
- Heel Pain (APMA)
📋 Dr. Tom Biernacki, DPM, FACFAS answers:
A protruding bone on the outside of the foot is most commonly a bunionette (tailor’s bunion) at the 5th metatarsal head, a bony spur, or — less often — a displaced or healing stress fracture. If it’s been there long-term and only hurts with shoes, conservative management (wider shoes, padding) usually resolves it. If it appeared suddenly, is tender to touch, or followed trauma, an X-ray is essential to rule out fracture.
Footwear & Orthotics for a Prominent Foot Bone
A bony prominence on the outside of the foot is often aggravated by tight shoes. See our podiatrist-recommended shoes with wide, soft uppers, and recommended orthotics to offload the area. Persistent pain warrants an in-office evaluation.

Specialist For This Condition
Dr. Carl Jay, DPM is the Balance Foot & Ankle reconstructive surgeon other doctors refer to when a protruding bone or 5th-metatarsal deformity needs surgical evaluation. Fellowship-trained in complex foot and ankle reconstruction. Book online or call (810) 206-1402 to schedule a consultation at the Howell or Bloomfield Hills office.
Related foot-bump guides
Other “bump or bone on the foot” guides worth comparing:
- Bump or lump on the side of the foot
- Bone sticking out on the outside of the foot
- Foot & ankle conditions hub
A bony prominence on the foot sometimes needs evaluation — see our guide to bunions & bone/toe deformities.
When the Bump Is Normal Anatomy and the Shoe Is the Problem
A useful thing to know before you worry too much: most of the prominences people find on the outer border of the foot are normal anatomy that has become symptomatic, not something that has grown. The styloid process at the base of the fifth metatarsal is a bony flare that everyone has, and in feet with a higher arch it simply sits more laterally and takes more pressure. It becomes painful when the counter of a shoe presses against it for hours a day. That distinction matters because it changes the treatment entirely — if the bone is normal and the shoe is the aggravator, the answer is the shoe, and no amount of stretching or icing will do the job.
- A firm prominence roughly halfway along the outer border, tender only where the shoe touches — this is the fifth metatarsal styloid, and it is the most common version of this complaint. It needs lateral width and a softer counter rather than treatment of the bone itself; shoes with genuine width through the midfoot and forefoot resolve the majority.
- The bump sits further forward, at the base of the little toe, with redness over it — that is a bunionette, or tailor’s bunion, and it is the fifth-toe counterpart of a bunion. Same principle: forefoot width is the intervention that matters.
- Aching along the outer border that builds with activity, tender behind and below the ankle bone — this points at the peroneal tendons rather than bone. Peroneal tendonitis is frequently mistaken for a bony problem because the tendons run directly over the prominence.
- You have a high arch and have rolled the same ankle more than once — that combination is the underlying driver in a good number of these cases. A rigid, supinating foot loads its outer border with every step, and the prominence is simply where that load concentrates. Footwear chosen for a supinating foot changes where the pressure goes.
- Tightness or pain tracking up from the outer heel into the Achilles — a tight calf increases lateral loading, and the two problems reinforce each other; see shoe selection when the Achilles is involved.
- The prominence appeared suddenly after twisting the ankle inward — this one is different in kind and should not wait. An inversion injury can avulse the base of the fifth metatarsal, and it is routinely treated as “just a sprain”. Footwear during a metatarsal fracture is a real part of healing, but the priority is getting it imaged first.
The practical test at home is simple: press the prominence directly with the shoe off. If it is tender to direct pressure but comfortable when you walk barefoot, the bone is fine and the shoe is doing the damage. If it hurts when you walk barefoot as well, something structural is loading it and that is worth examining properly. We can usually settle which it is in a single visit — our Howell and Bloomfield Township offices are at (810) 206-1402.
Get the Bump on the Side of Your Foot Identified
Most of these turn out to be normal anatomy that a better-shaped shoe will quiet down, and we will tell you plainly when that is the case rather than manufacturing a treatment plan. But the list above contains two things you cannot afford to sit on — a fifth metatarsal fracture that is a Jones rather than an avulsion, and a new prominence on a neuropathic foot — and neither can be ruled out by looking at it. An X-ray in the office settles the first question in a few minutes.
Book as a new patient at our Howell podiatry office or our Bloomfield Township office, or call (810) 206-1402. Bring the shoes you wear most, including your work shoes — when the bump is a pressure problem, the shoes are usually holding the answer.
Book an appointment with a podiatrist
A prominent bone on the outside of the foot can be a tailor’s bunion, an extra bone present since childhood, or the healed remains of an old fracture — and they are managed very differently. A weight-bearing X-ray settles which one it is in a single visit. Balance Foot & Ankle sees patients at two offices — Howell in Livingston County, and Bloomfield Township in Oakland County.
Book online, 24/7: choose a real appointment time at Howell or Bloomfield Township. Prefer to speak with someone first? Call (810) 206-1402 or use the form below.
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.