

Capsulitis of the second toe — pain at the base of the second toe that worsens with walking — responds to a specific buddy-taping technique that takes pressure off in seconds.
You’ve come to the right podiatry team. Dr. Tom Biernacki, DPM, FACFAS — board-certified foot & ankle surgeon with 3,000+ surgeries — explains exactly what capsulitis of the second toe taping means and what works. Call (810) 206-1402 for same-day appointment at Howell or Bloomfield Hills.
Capsulitis of the second toe is a plantar plate injury — and the taping direction relative to the toe’s drift pattern determines whether the tape offloads the injured ligament or stresses it further. Most taping guides show one method. The correct method depends on which direction the second toe has started to deviate, and whether the plantar plate is partially or fully torn. Getting this wrong accelerates the crossover toe deformity that capsulitis leads to if untreated. Call (810) 206-1402 or book online — we tape and assess plantar plate integrity on the first visit.

- COMFORTABLE SUPPORT: 1/4 inch thick felt metatarsal pads provide gentle cushioning under the ball of the foot for daily wear
- VALUE PACK: Includes 6 pairs (12 pieces) to ensure long-lasting comfort and convenience
- ADHESIVE BACKING: Strong adhesive keeps the pad in place inside shoes or directly on the foot
- MADE IN THE USA: Proudly designed, cut, and manufactured in the United States
- EASY TO CUSTOMIZE: Can be trimmed with scissors for a better fit inside a variety of footwear
As an Amazon Associate, Balance Foot and Ankle earns from qualifying purchases. Product links are affiliate links and we may earn a commission at no extra cost to you. This does not influence our clinical recommendations. Last update on 2026-07-26 / Images from Amazon Product Advertising API
Medically reviewed by Dr. Tom Biernacki, DPM
Board-certified podiatric surgeon | Balance Foot & Ankle | Last reviewed: May 2026
Second toe capsulitis is one of those conditions that improves dramatically with the right taping technique — and worsens with the wrong one. As a podiatrist who treats this regularly, I want to show you exactly how we tape for capsulitis and why it works so well as part of a broader conservative treatment program.
What Is Capsulitis of the Second Toe?
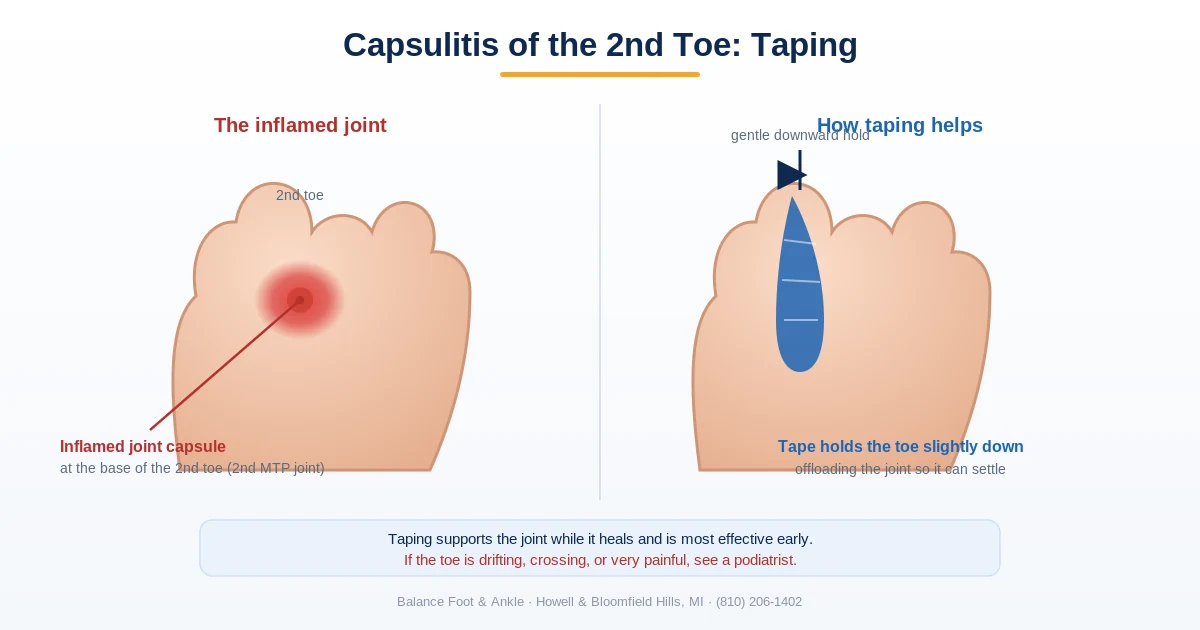
Capsulitis is inflammation of the joint capsule and plantar plate at the second metatarsophalangeal (MTP) joint — the joint at the base of the second toe. It’s caused by chronic overloading of this joint, usually because the first ray (big toe and its metatarsal) is insufficient at absorbing push-off forces due to a short first metatarsal, hallux valgus, or first ray hypermobility. The result is that the second metatarsal bears disproportionate load, stressing the capsule and plantar plate with every step. If not treated, the plantar plate tears progressively and the second toe drifts upward and medially into a crossover toe deformity — a much harder problem to fix.
How to Tape for Second Toe Capsulitis
The goal of taping is to hold the second toe in slight plantarflexion (pointing downward), which reduces tension on the dorsal capsule and plantar plate and allows the inflamed tissue to rest and heal during walking. This is often called “plantar plate taping” or “hammertoe taping” and is one of the most effective conservative tools for grades I and II capsulitis.
- Materials: Rigid athletic tape (1 inch width) or Leukotape P cut into 6-inch strips. Foam underwrap (Prewrap) to protect skin if used daily. Toe spacer foam if the toe is drifting medially.
- Step 1 — Anchor: Wrap a strip of tape around the base of the second toe (proximal phalanx), overlapping slightly onto the third toe for stability.
- Step 2 — Plantarflexion hold: With the second toe held in slight downward (plantarflexed) position, run a strip of tape from the dorsal anchor, under the ball of the foot, and secure on the plantar surface of the foot. This creates a sling that holds the toe in the correct position.
- Step 3 — Reinforce: Apply a second reinforcing strip in the same direction. The toe should feel firmly held but not compressed or numb.
- Duration: The tape can be worn during waking hours and replaced every 1–2 days. Continue for 4–8 weeks as part of a complete rehabilitation program.
- Check: The taped toe should have full circulation (pink color, no numbness). If the toe turns white, blue, or numb, loosen immediately.
Key takeaway: Taping alone does not cure capsulitis — it reduces symptoms while the underlying mechanics are corrected. Without addressing the first ray insufficiency (with a custom orthotic) and reducing overloading activity, capsulitis will return when taping is discontinued.
Complete Treatment Program for Capsulitis
Taping works best as part of a multi-component protocol. Here is the complete program we use at Balance Foot & Ankle for second MTP capsulitis Grades I–III.
- Taping (plantar plate taping): As described above — reduces load on the plantar plate and capsule during daily walking.
- Metatarsal pad: A teardrop-shaped metatarsal pad placed just proximal to the second metatarsal head redistributes weight proximally, off the MTP joint.
- Custom orthotic: Addresses first ray hypermobility or short first metatarsal — the root cause in most patients. A properly prescribed custom orthotic significantly reduces recurrence compared to taping alone.
- Activity modification: Avoid barefoot walking on hard surfaces, high heels (>1.5 inches), and activities that involve prolonged second toe dorsiflexion (such as lunges and deep squats) during the acute phase.
- Wide, stiff-soled footwear: Limits the degree of MTP dorsiflexion during gait, reducing plantar plate stress.
- Corticosteroid injection: For Grades II–III with significant synovitis — ultrasound-guided injection into the second MTP joint reduces inflammation rapidly. We limit to 1–2 injections due to plantar plate atrophy risk with repeated cortisone.
- Surgery: Reserved for Grade III–IV capsulitis with established plantar plate tear and crossover deformity. Plantar plate repair or flexor-to-extensor tendon transfer restores alignment.
⚠️ See a podiatrist if:
- The second toe is visibly drifting toward or crossing the big toe (Grade III–IV)
- The Lachman’s test is positive (toe can be pulled upward significantly)
- Pain persists after 6 weeks of taping and orthotic use
- The second toe feels “loose” or like it might dislocate
Taping a drifting second toe buys time — it doesn’t hold it
Tape and a metatarsal pad genuinely reduce capsulitis pain, and for an early, stable toe they can be enough. What they can’t do is stop a plantar plate that’s actually tearing. Once the second toe starts drifting toward the big toe or lifting out of line with the others, the ligament underneath has usually given way, and that doesn’t reverse with taping — it progresses. If your toe has visibly moved rather than simply hurting, it needs examining while the correction is still simple.
Howell — 4330 E Grand River Ave, Howell MI 48843 · Bloomfield Hills — 43494 Woodward Ave #208, Bloomfield Hills MI 48302
The Most Common Mistake We See
The most common mistake is taping in the wrong direction — pulling the toe upward (dorsiflexion) instead of downward (plantarflexion). We regularly see patients who have been taping for weeks without improvement because they were holding the toe in the very position that stresses the plantar plate. The toe must be held slightly down and toward the plantar surface to off-load the inflamed structure.
Medi-Dyne Tuli’s Cheetah Metatarsal Pad
⭐ 4.5★ | 12K+ Sold
Essential for capsulitis of the second toe — offloads the 2nd metatarsophalangeal joint and reduces the painful pressure on the joint capsule.
PowerStep Pinnacle Arch Support Insoles
⭐ 4.7★ | 50K+ Sold
Supports the entire metatarsal arch during capsulitis recovery — reduces the excessive extension forces that tear the joint capsule.
DIFFERENTIAL DIAGNOSIS — CONDITIONS THAT MIMIC CAPSULITIS
- Morton’s neuroma — burning/tingling between toes vs. dorsal joint swelling; distinguished by Mulder’s click test
- Plantar plate tear (Grade III–IV) — capsulitis that has progressed; toe deviates medially, no longer reducible
- Freiberg’s infraction — 2nd metatarsal head avascular necrosis; shows on X-ray as flattened head
- Stress fracture of 2nd metatarsal — pain along shaft, not at the MTP joint; bone scan or MRI confirms
- 2nd toe hammertoe — secondary deformity from longstanding capsulitis; requires different taping approach
Frequently Asked Questions
How long should I tape my second toe for capsulitis?
Tape daily during waking hours for 4–8 weeks, or until the joint is pain-free with weight-bearing. Discontinue gradually — don’t stop abruptly. Transition to an orthotic with metatarsal pad for ongoing support.
Can second toe capsulitis heal without surgery?
Yes — Grades I and II capsulitis respond very well to conservative care with taping, orthotics, and activity modification. Grade III with plantar plate tear and crossover deformity often ultimately requires surgery for definitive correction, though conservative care can manage symptoms for years.
What is the difference between capsulitis and a neuroma?
Capsulitis produces dorsal joint swelling, MTP joint tenderness, and positive Lachman’s test — pain is at the joint. Morton’s neuroma produces burning, tingling, and numbness in the web space between toes — pain is between the metatarsal heads, not at the joint, and the Mulder’s click test reproduces it.
RED FLAGS — WHEN TAPING ISN’T ENOUGH
- 2nd toe crossing over or under the hallux — Grade III/IV tear, needs surgical evaluation
- No improvement after 6–8 weeks of taping and orthotics
- Significant swelling that worsens with activity despite offloading
- Numbness or tingling with MTP joint pain (concurrent neuroma possible)
- Prior corticosteroid injection with recurrence — plantar plate may be ruptured
If any of these apply, call (810) 206-1402 for advanced imaging and treatment planning.
The Bottom Line
Plantar plate taping for second toe capsulitis is simple, effective, and a foundational part of our conservative treatment protocol. When done correctly (toe slightly plantarflexed, not dorsiflexed), it dramatically reduces daily pain and allows the capsule to heal. Combined with orthotics and footwear changes, the majority of Grade I–II capsulitis cases are fully resolved within 6–10 weeks. Come see us at Balance Foot & Ankle in Howell or Bloomfield Hills if your second toe pain persists.
Sources
- Coughlin MJ. Second metatarsophalangeal joint instability in the athlete. Foot Ankle. 1993.
- Bouché RT, Heit EJ. Combined plantar plate and hammertoe repair with flexor digitorum longus tendon transfer for chronic, severe sagittal plane instability of the lesser metatarsophalangeal joints. J Foot Ankle Surg. 2008.
- Thompson FM, Hamilton WG. Problems of the second metatarsophalangeal joint. Orthopedics. 1987.
- AAOS. “Metatarsalgia.” OrthoInfo.
- Coughlin MJ, et al. “Crossover second toe deformity.” Foot Ankle Int. 2011.
Ready to Get Relief?
Same-day appointments available in Howell & Bloomfield Hills, MI
4.9★ | 1,123 Reviews | 3,000+ Surgeries
Or call: (810) 206-1402
Frequently Asked Questions
When should I see a podiatrist?
If symptoms persist past 2 weeks, affect your normal activity, or are accompanied by red-flag symptoms (warmth, redness, swelling, inability to bear weight).
What does treatment cost?
Most diagnostic visits and conservative treatments are covered by Medicare and major insurers. Out-of-pocket costs vary by your specific plan.
How quickly can I get an appointment?
Most non-urgent cases see us within 5 business days. Urgent cases (sudden pain, possible fracture) typically same or next business day.
Dr. Tom’s Recommended Products to Use with Capsulitis Taping
- PowerStep Pinnacle Insoles — Use alongside taping for comprehensive second MTP offloading. Metatarsal support built into the Pinnacle arch reduces joint stress even when taping isn’t practical (at work, in dress shoes).
- Foot Petals Tip Toes Cushions — For women’s shoes: targeted cushioning under the second metatarsal head as a taping alternative in dress footwear where athletic tape isn’t visible or comfortable.
- Doctor Hoy’s Natural Pain Relief Gel — Apply to the second MTP joint before taping to reduce the baseline inflammation driving the pain.
Capsulitis requiring daily taping to walk without pain has likely progressed to plantar plate damage — this needs professional evaluation. Book a same-day appointment → · (810) 206-1402
In-Office Treatment at Balance Foot & Ankle
If home treatment isn’t resolving your capsulitis of the second toe, our podiatry team at Balance Foot & Ankle can help. We offer same-day evaluations and advanced in-office treatments to get you back on your feet faster.
Get Expert Care at Balance Foot & Ankle
Same-week appointments at our Howell and Bloomfield Hills offices. Board-certified podiatric surgeons. Most insurance accepted.
What is capsulitis of the second toe?
Capsulitis of the second toe is inflammation of the joint capsule surrounding the second metatarsophalangeal (MTP) joint, causing pain and swelling in the ball of the foot just behind the second toe. It results from chronic overloading of the joint — common in people with a long second metatarsal, bunion (which transfers load to the second MTP), high-heeled shoes, or activities requiring repeated toe extension. Left untreated, it can progress to plantar plate tear and second toe dislocation.
How do you tape capsulitis of the second toe?
The standard taping technique loops a 1-inch athletic tape strip under the second toe, wraps it proximally toward the foot, and secures it to limit dorsiflexion (upward bending) at the MTP joint. This reduces plantar plate stress during push-off. A podiatrist-taught buddy taping technique (taping the 2nd to 3rd toe) provides lateral stability. Kinesiology tape can also be applied in a ‘Y’ shape around the MTP joint to reduce swelling.
How long does capsulitis of the second toe take to heal?
Mild capsulitis resolves in 6–8 weeks with taping, metatarsal pad offloading, and modified footwear. Moderate cases with plantar plate strain take 3–6 months. Severe cases with plantar plate tear may require 6–12 months of conservative care, and surgical repair is considered for complete tears with toe dislocation. Early treatment is critical — the longer capsulitis goes untreated, the more likely progressive toe deformity becomes.
What shoes are best for capsulitis of the second toe?
Shoes with a stiff or rocker-bottom sole are most beneficial, as they reduce MTP joint extension during push-off. A wide, deep toe box prevents lateral compression. Avoid high heels, which place the MTP joint in prolonged extension and increase plantar plate load by up to 75%. Shoes that accommodate a metatarsal pad — placed just behind (proximal to) the second metatarsal head — provide the most effective offloading strategy.
Capsulitis often progresses to toe drift and the “daylight sign” — a key visual indicator of joint instability. See our guide: Toes Separating: The Daylight Sign and What It Means.
How is capsulitis of the second toe different from Morton’s neuroma?
Both cause pain in the ball of the foot, and they are commonly confused. Capsulitis is inflammation of the joint capsule at the second metatarsophalangeal (MTP) joint, so the pain sits directly over that one joint, worsens when you push off, and is often paired with swelling and a sense that the toe is drifting or unstable. Morton’s neuroma is an irritated nerve between the metatarsal heads — most often the third and fourth — and it causes burning, tingling, or numbness that radiates out into the toes rather than pinpoint tenderness on a joint. A podiatrist can usually tell them apart on examination.
Does taping help capsulitis of the second toe?
Yes. Buddy taping or specific capsulitis taping techniques stabilize the toe joint, reduce stress on the inflamed capsule, and can significantly decrease pain during walking. Taping is most effective when combined with orthotics and activity modification.
How long does second toe capsulitis take to heal?
With conservative treatment — including taping, custom orthotics, and reduced high-impact activity — most cases improve within 6–12 weeks. Left untreated, capsulitis can progress to toe dislocation, requiring more extensive intervention.
How does taping help capsulitis of the second toe?
Taping for second-toe capsulitis works by buddy-splinting the second toe to the third in a slightly plantarflexed (downward) position. This reduces dorsiflexion stress on the plantar plate at the 2nd MTP joint — the primary damage mechanism in capsulitis. When the toe is taped down, the plantar plate is offloaded during the propulsive phase of gait, allowing the ligament to heal without constant re-injury. Taping also reduces the ‘floating toe’ deformity that develops when the plantar plate tears and the toe drifts upward.
What type of tape works best for second-toe capsulitis?
1-inch medical paper tape (3M Micropore or similar) is most commonly used for second-toe buddy taping due to its flexibility and skin-friendliness for long-term use. Kinesiology tape (KT Tape or Rocktape) is an alternative for patients who need to maintain taping for 3-5 days at a time. The key is placement: the tape must hold the toe in mild plantarflexion without cutting off circulation — the toe tip should retain normal color and feel with the tape applied. Podiatrists often show patients how to tape before initiating other treatments.
When should I see a podiatrist for capsulitis of the second toe?
See a podiatrist if symptoms persist beyond 4 weeks, limit normal activity, or you have diabetes or poor circulation. Same-day appointments at Balance Foot & Ankle — (810) 206-1402 — Howell & Bloomfield Hills, MI.
For a complete clinical overview: Our Complete Plantar Fasciitis & Forefoot Treatment Guide — covers causes, diagnosis, treatment protocols & exercises from a Michigan board-certified podiatrist.
Footwear & Orthotics for Second-Toe Capsulitis
Stiff-soled shoes and metatarsal-pad orthotics offload the inflamed joint at the base of the second toe. See our podiatrist-recommended shoes, and book an evaluation if pain persists beyond a few weeks.
Second-toe pain that keeps coming back?
Taping calms capsulitis, but recurring pain usually needs offloading and a real treatment plan. In Michigan? Our podiatrists treat the root cause before the toe drifts. Same-week visits in Howell & Bloomfield Hills.
📅 Book an Appointment 📞 (810) 206-1402★ 4.9 from 1,123+ Google reviews · Same-week visits · We verify your insurance free — most visits are just a copay.
Book an appointment with a podiatrist
Taping holds the toe in position while the capsule calms down, but untreated capsulitis tends to progress — the ligament stretches out and the toe begins to drift across its neighbour, which is far harder to correct than the inflammation that preceded it. Early assessment is what keeps this reversible. Balance Foot & Ankle sees patients at two offices — Howell in Livingston County, and Bloomfield Township in Oakland County.
Call (810) 206-1402 or use the form below and our team will find you an appointment time.
Dr. Tom Biernacki, DPM is a board-certified foot & ankle surgeon (ABFAS & ABPM) at Balance Foot & Ankle Specialists in Southeast Michigan. With over a decade of clinical experience, he specializes in heel pain, bunions, diabetic foot care, sports injuries, and minimally invasive surgery. Dr. Biernacki is a member of the APMA and ACFAS, and his patient education content on MichiganFootDoctors.com and YouTube has made him one of the most-followed foot & ankle educators on YouTube.